Article Text

Abstract
Background A pretrial clinical improvement project for the BOOST-II UK trial of oxygen saturation targeting revealed an artefact affecting saturation profiles obtained from the Masimo Set Radical pulse oximeter.
Methods Saturation was recorded every 10 s for up to 2 weeks in 176 oxygen dependent preterm infants in 35 UK and Irish neonatal units between August 2006 and April 2009 using Masimo SET Radical pulse oximeters. Frequency distributions of % time at each saturation were plotted. An artefact affecting the saturation distribution was found to be attributable to the oximeter's internal calibration algorithm. Revised software was installed and saturation distributions obtained were compared with four other current oximeters in paired studies.
Results There was a reduction in saturation values of 87–90%. Values above 87% were elevated by up to 2%, giving a relative excess of higher values. The software revision eliminated this, improving the distribution of saturation values. In paired comparisons with four current commercially available oximeters, Masimo oximeters with the revised software returned similar saturation distributions.
Conclusions A characteristic of the software algorithm reduces the frequency of saturations of 87–90% and increases the frequency of higher values returned by the Masimo SET Radical pulse oximeter. This effect, which remains within the recommended standards for accuracy, is removed by installing revised software (board firmware V4.8 or higher). Because this observation is likely to influence oxygen targeting, it should be considered in the analysis of the oxygen trial results to maximise their generalisability.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://adc.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Preterm infants often require supplemental oxygen for prolonged periods. There is considerable interest in the effect of oxygen therapy on morbidity and mortality in these infants.1,–,6 For more than 60 years there has been insufficient evidence to guide treatment and this is now the subject of an international group of randomised trials. The aim of these trials is to compare the outcomes of extremely preterm infants who have their pulse oximeter saturation (SpO2) maintained in either the range 85–89% or 91–95% until they reach 36 weeks corrected gestational age. The trials are using Masimo SET Radical pulse oximeters (Masimo, Irvine, California, USA). These oximeters were chosen because they were in widespread use when the trials were planned and are popular because of their ability to measure during patient motion and in circumstances of low perfusion. The trials were made possible by the assistance of Masimo Corporation who provided modified oximeters to enable a masked comparison between the trial groups.
What is already known on this topic
▶ Different oxygen targeting practices may influence the short and long term outcomes of preterm infants.
▶ International trials are being conducted with the aim of ending 60 years of uncertainty about oxygen therapy for preterm infants.
What this study adds
▶ A software characteristic causes the Masimo SET Radical oximeter to return fewer saturation values between 87% and 90% and an excess of higher values.
▶ This may affect oxygen targeting and can be removed by installing revised software (board firmware V4.8 or higher).
▶ The international trials will produce a pooled result that is widely generalisable.
Prior to commencing the BOOST-II UK trial (https://www.npeu.ox.ac.uk/boost), participating units provided routine care to convalescent oxygen dependent preterm infants using standard unmodified Masimo SET Radical oximeters and participated in a pretrial audit to evaluate and support their success in saturation targeting. During this audit, SpO2 data were recorded in the oximeters and were downloaded for analysis and feedback to the clinical teams. In the course of this analysis, it was noted that the frequency histograms of the SpO2 readings had an unexpected appearance. The purpose of this report is to describe the observation and discuss its relevance to clinical practice and the oxygen saturation targeting trials.
Methods
SpO2 data were gathered from 176 oxygen dependent preterm infants in 35 UK and Irish neonatal units between August 2006 and April 2009. Monitoring was performed for normal clinical indications using standard, unmodified Masimo SET Radical oximeters. Care was guided by these oximeters for a period of up to 2 weeks. During this time, the SpO2 data were recorded by the oximeter every 10 s. The infants were being given standard care by regular neonatal unit staff using standard equipment with no additional interventions or observations. As this was an audit of normal care for quality improvement purposes, parental consent was not obtained and ethics committee approval was not required. At the end of the period of care, the SpO2 data were downloaded and fed back to the clinical team so that the staff could evaluate their success with saturation targeting. The feedback was provided as bar charts describing the time spent in different saturation ranges.
Alternative ways of describing the data were explored and the SpO2 data were later plotted in the form of frequency histograms of the percentage of SpO2 readings at each saturation. When the saturation distributions were reviewed and appeared to have an artefact modified appearance, work was undertaken by Masimo Corporation to explain the findings. The explanation lay in the oximeter software algorithm. A revised software algorithm was supplied by Masimo Corporation and installed into the oximeters. Paired studies comparing the saturation distributions returned by Masimo oximeters running the new software algorithm with commercially available oximeters from four other manufacturers were conducted on a series of preterm infants cared for in the neonatal unit of the Royal Infirmary of Edinburgh, UK. Written parental consent was obtained for each of the paired comparisons and the protocol for the paired comparisons was reviewed by the Lothian Research Ethics Committee who determined that a full ethics application and review was not required because the study was an equipment evaluation with no modification to patient care other than the attachment of an additional oximeter. Probes from both oximeters were sited postductally for these comparisons.
Results
Pretrial audit data were obtained from 176 preterm infants; all were receiving supplemental oxygen at the time of study. Detailed clinical information was not gathered as the audit was not intended as a research study. Figure 1A shows the frequency histogram of saturation readings from one infant. The distribution has an artefactual appearance, with a large dip in the histogram due to a lower frequency of SpO2 readings in the range 87–90% than would be expected from the remainder of the distribution. It looked as if there were missing values. This appearance was identifiable in almost all histograms from individual infants. The area of apparently missing data always fell in the range 87–90%. The size of the area of missing values depended on the distribution of the remaining values. Where an SpO2 of 87–90% was in the middle of the patient's distribution, the dip appeared large. Where the centre of the distribution was above a saturation of 90% so that values of 87–90% were in the tail, the dip appeared smaller. In a few cases with very high SpO2 values, the dip was not apparent as there were too few values in the range 87–90%. This is shown in figure 1B where histograms from five infants have been plotted, and in figure 1C where pooled data from all 176 audits have been combined, showing the overall effect on the saturation distribution of oxygen dependent preterm infants cared for using this oximeter.

Frequency histograms for proportion of time spent at each saturation value while receiving supplemental oxygen in infants monitored using un-modified Masimo SET Radical pulse oximeters: (A) individual infant; (B) five individual infants; (C) cumulative data for all 176 infants in the prospective audit.
Explanation
We are grateful to Masimo Corporation for promptly identifying the explanation. Oximeters determine saturation by measuring the ratio of red to infrared waveform intensities detected by the oximeter sensor (figure 2) and use a calibration curve to convert these ratios into saturation values. In development, this conversion is validated against arterial blood samples measured by a CO-oximeter. The reduced frequency of SpO2 values of 87–90% is due to the calibration algorithm used by the oximeter. Inspection of the calibration curve in the area corresponding to SpO2 values of 87–90% shows a transition where the slope of the curve becomes steeper for a short section. The calibration curve has been generated by merging two separate curves and the change in slope is the move from one curve to the other. Where the slope is steeper, the SpO2 value returned increases more for each change in light ratio than would otherwise have been the case on either curve so that SpO2 readings of 87–90% become less frequent. From a SpO2 of 87% upwards, as the lower curve climbs to join the higher curve, SpO2 reads progressively a little higher than would be the case with the lower curve. This leads to an artefactual elevation of SpO2 readings that is maximal at a displayed value of 90% and is around 1.6% higher (effectively up to 2% because oximeters display whole numbers). This elevation gradually reduces in size as SpO2 increases further until it is no longer present at SpO2 values above 96%.

Plot of the ratio of red to infrared wavelength intensities and corresponding oxygen saturation (data supplied by Masimo Corporation).
The manufacturers indicate that the upper curve was used to provide saturation readings consistent with the tendency of manufacturers at the time that the oximeter was originally produced to adjust saturations in the 90s upwards a little to obviate the effects of low levels of circulating variant haemoglobins. They added the lower curve, which is free of upward adjustment, in 2002 as newborn preterm infants were being targeted to lower saturations. The effect of this ‘dual’ curve is that the saturation values that are missing from the distribution in the region of 87–90% have been shifted upwards by up to 2% and there is a corresponding increase in the frequency of higher values.
Figure 3 shows SpO2 data gathered from an oxygen dependent preterm baby who was being cared for using a Nellcor Oximax N600x oximeter (Covidien-Nellcor, Boulder, Colorado, USA). The baby also had an unmodified Masimo SET Radical pulse oximeter attached, and the two simultaneous saturation profiles show the reduced number of values of 87–90% in the Masimo histogram and the higher number of SpO2 readings of 91–96% that were obtained with the Masimo oximeter.

Frequency histograms for proportion of time spent at each saturation value while receiving supplemental oxygen: (A) infant cared for using a Nellcor OxiMax N-600x oximeter with Nellcor OxiMax probe (Covidien-Nellcor, Boulder, Colorado, USA) and simultaneously monitored using a Masimo SET Radical oximeter with a Masimo LNOP NeoPt-L probe; (B) infant cared for using a Masimo SET Radical oximeter with the revised software algorithm and simultaneously monitored with a Masimo SET Radical oximeter with the original software algorithm.
Masimo Corporation supplied new software with a revised conversion algorithm (board firmware V4.8 or higher) that relied on a single calibration curve and this was installed into all BOOST-II UK trial oximeters in December 2008. Figure 3B shows a paired comparison of saturation readings obtained from an oxygen dependent preterm infant cared for using an oximeter with the new saturation algorithm and simultaneously monitored with a standard Masimo SET Radical oximeter with the original algorithm.
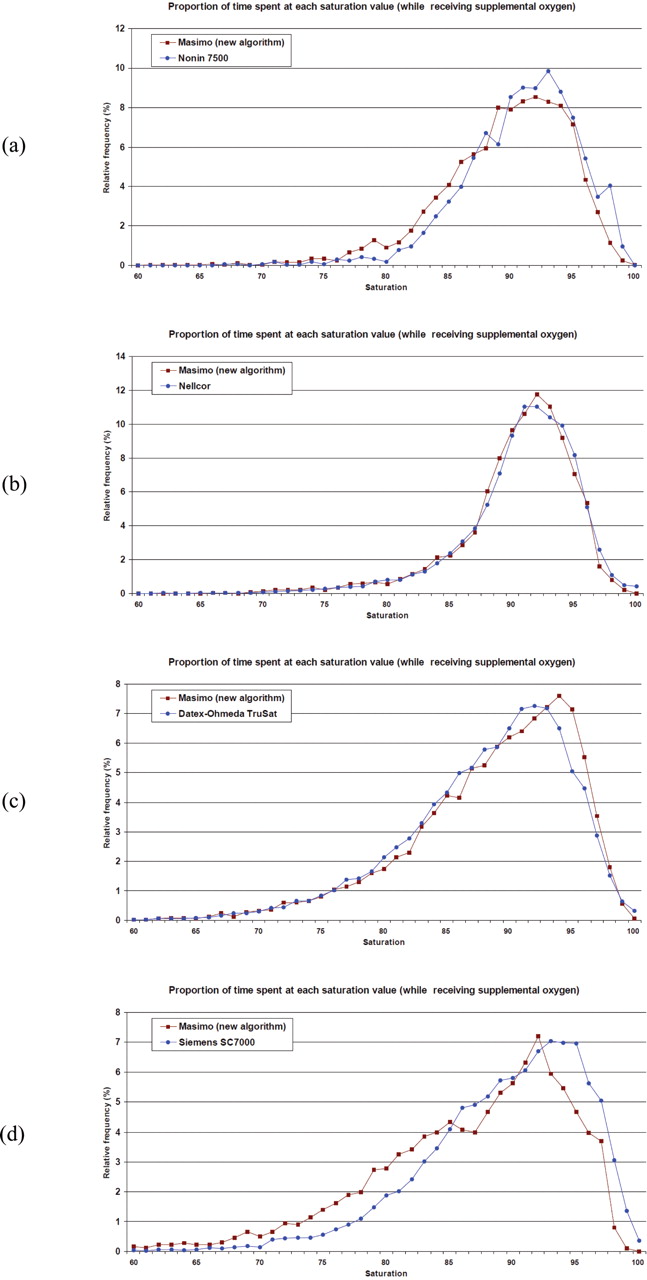
Figure 4 shows paired comparisons of SpO2 values obtained from four infants whose clinical care was guided by one of four different current commercially available oximeters and who also had SpO2 data gathered simultaneously with a Masimo SET Radical oximeter with the revised software. The revised Masimo software returned a distribution that was similar to that of the other four oximeters.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Frequency histograms for proportion of time spent at each saturation value while receiving supplemental oxygen for infants cared for using four commercially available oximeters and simultaneously monitored with a Masimo SET Radical oximeter with the revised software algorithm and a Masimo LNOP NeoPt-L probe: (A) Nonin 7500 using a 7000N Neonatal Flexiform II probe (Nonin Medical, Plymouth, Minnesota, USA); (B) oximeter with Nellcor OxiMax probe (Covidien-Nellcor, Boulder, Colorado, USA); (C) Datex-Ohmeda TruSat with an OxyTip sensitive skin probe (GE Healthcare, Chalfont St Giles, UK); (D) Siemens SC7000 (Siemens UK, Frimley, UK) with a Nellcor OxiMax probe.
Discussion
We have shown that when it is used to monitor preterm infants receiving supplemental oxygen, the Masimo SET Radical pulse oximeter returns a reduced number of values of 87–90%. This is explained by the internal calibration algorithm, which changes in this region and adjusts SpO2 values above 87% upwards. A new software algorithm removed this artefact and returns a distribution of values that is similar to other current oximeters.
According to the product information, the oximeter is validated for accuracy in human blood studies on healthy adult volunteers in induced hypoxia studies in the range of 70–100% SpO2 against a laboratory CO-oximeter. This variation equals ±1 SD, which encompasses 68% of the population. The stated accuracy for neonates is ±3%, so by this standard at least 68% of the time the displayed SpO2 reading should be within ±3% of the simultaneous CO-oximeter value on an arterial blood sample. In this regard the original oximeter performs within all recommended accuracy standards.
Where SpO2 is targeted over a wide range, including values of 87% and 95%, this artefact is not likely to be of clinical significance. However, oximeters are sometimes used to target a narrower range or to determine a threshold saturation.7,–,9 Under these circumstances the effect could be greater. Oximeters are used as a screening tool to identify borderline saturations in congenital heart disease.10 11 Some cases of duct dependent systemic circulation are not identified by this approach. It is possible that a slight artefactual elevation of saturation between 87% and 95% could mask some cases. It is becoming usual for bronchopulmonary dysplasia to be categorised by whether or not a saturation of 90% is maintained breathing air.12,–,14 An artefactual increase in SpO2 from 89% to 91% would result in fewer infants being categorised as having bronchopulmonary dysplasia and might influence the duration of supplemental oxygen exposure.
In the neonatal oxygen trials, infants have been targeted using modified Masimo Radical SET oximeters to maintain saturations either in the range 85–89% or 91–95%.15 This artefact in the algorithm would be expected to reduce the number of saturation values in the target range in the group targeted to lower saturations. This might make this lower saturation target group harder to maintain within range, leading to more oxygen adjustments and greater variability in saturation, including time spent with high or low saturations.
When these observations were explained, Masimo Corporation provided the revised software, which eliminated the artefact, removing the deficit of values in the range 87–90%, and reducing the uplift in saturations. With assistance from Masimo the new software algorithm was installed into the oximeters of the BOOST-II UK trial in December 2008 and into the Australian and Canadian oxygen trial oximeters in early 2009, so that the final results of the international collaboration will be as generalisable as possible to current oximeters from Masimo and other manufacturers.
The SUPPORT trial was the first of the oxygen trials to complete recruitment. Outcomes to hospital discharge were published recently.9 There was a large and highly significant reduction in retinopathy of prematurity in the group who had their oxygen saturation targeted lower. The same group showed a slight excess of mortality, of borderline conventional statistical significance. The data monitoring committees of the ongoing trials in the UK, Australia and New Zealand and Canada reviewed their individual trial data in light of the SUPPORT trial results and independently recommended continuing recruitment to all three trials. The SUPPORT trial was completed before the oximeter modifications. Because the ongoing trials began evaluating an intervention that results in different saturation distributions, it is critically important to the generalisability of the trial results that a pooled analysis of the data should describe outcomes using either algorithm.
In conclusion, we have shown that the algorithm used by one generation of the Masimo SET Radical oximeter returns a distribution of saturation values above 87% that is different from other oximeters. This could be important if the device is being used to target saturation values in a narrow range or to evaluate threshold saturation values. This finding has important implications for the interpretation of emerging evidence in neonatal intensive care.
Acknowledgments
The authors are grateful to the nursing staff and neonatologists of the units participating in the BOOST-II UK trial for contributing to the pretrial quality improvement exercise and enabling this important information to be identified and corrected. The authors thank Masimo Corporation for enabling the trials to take place and for promptly explaining the oximeter observations and providing the revised software.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.