
Abstract
Objective
Volume-targeted modes are designed to deliver a constant tidal volume (Vt) at lowest possible pressure independently of changes in compliance, resistance, and leak of the respiratory system. We examined whether these volume-targeted modes respond rapidly enough to sudden changes in respiratory mechanics (e.g., selective intubation, surfactant administration, endotracheal tube kinking, de-kinking, obstruction), resulting in insufficient or excessive Vt delivery.
Design and setting
Bench study of six neonatal ventilators in the volume-targeted mode simulating preterm and full-term infant settings on a test lung.
Measurements and results
Breath-to-breath expiratory Vt were measured after rapid compliance, resistance, and leak changes. Under our test settings all ventilators showed important volume overshooting following rapid increase in compliance or decrease in resistance. Between one and 16 inflations were required to return to the set Vt. Some ventilators delivered inaccurate Vt under steady state condition while others showed considerable breath-to-breath Vt variability.
Conclusions
We observed inaccurate Vt delivery under specific conditions as well as immediate and sometimes prolonged volume overshooting after a rapid respiratory system compliance increase or resistance decrease in volume-targeted modes of modern neonatal ventilators. Similar discrepancies between the set Vt and the delivered inflations can be harmful in clinical situations, especially in newborns. Their clinical relevance needs to be clarified with safety studies in the neonatal population and we encourage manufacturers to further improve the ventilators algorithms.
Similar content being viewed by others

Introduction
Chronic lung disease, or bronchopulmonary dysplasia, is in part thought to be a result of injurious ventilation (i. e., ventilator-induced lung injury, VILI) [1]. Limitation of tidal volumes (Vt, i. e., low Vt ventilation) has proved to be an effective tool to attenuate VILI [2, 3] and to improve outcome in the clinical setting [3]. For neonates pressure-limited ventilation has been the traditional mode of ventilation for over three decades for two major reasons: (a) pressure limitation has allowed minimizing the risk of gross air leak (i. e., pneumothorax) and (b) technical limitations were given for reliable measurements of very small Vt. With the advent of small Vt ventilation as a lung-protective strategy and technological progress in the design of ventilators and pneumotachographs, volume-targeted modes [4] have been incorporated in many neonatal ventilators. These modes adapt peak inspiratory pressure (PIP) or inspiratory flow to the compliance and resistance of the patient's respiratory system in order to deliver the set Vt at the lowest possible airway pressure. The governing algorithm varies from one ventilator to the other. Some use the measured Vt (expiratory or inspiratory, depending on the algorithm) of the previous, others of the current inflation to feedback the measured PIP. This feedback may affect the adequacy of Vt delivery upon rapid changes in compliance (e.g., exogenous surfactant administration, right main stem bronchus intubation, acute constitution or drainage of pneumothorax, and reopening of atelectasis), resistance (e.g., kinking and de-kinking of the endotracheal tube or its obstruction by secretion or meconium), and airway leak (e.g., variable endotracheal tube leak depending on infant's head position).
Many potential advantages of volume-targeted over pressure-controlled ventilation in neonates have been reported in the literature [5, 6, 7, 8, 9, 10, 11, 12, 13, 14]: Breath-to-breath variability of Vt has shown to be reduced [6, 7, 9, 10] and PIP and mean airway pressure to be lowered [5, 8, 13, 14]. Slower respiratory rates have been observed, but the underlying mechanism of this remains unclear so far [8, 10]. Decreased lung inflammatory response and cytokine production has been found [7, 14], probably due to decreased shear stress to the lung tissue, acceleration of weaning from mechanical ventilation has been reported [11, 12], and a lower incidence of intraventricular hemorrhage or intraparenchymal brain echodensities has been observed than with intermittent mandatory ventilation (synchronized or not) in pressure-controlled mode [11, 12], potentially due to the lower airway pressure and decreased repercussions on cerebral blood flow by the more stable Vt.
On the other hand, Abubakar et al. [6] have noted substantial Vt fluctuations around the set value in clinical settings, which was attributed to the breath-to-breath variability of the infants' respiratory effort and the incapacity of this ventilator mode to adjust its support instantaneously. Others have warned of the latency of Vt adaptation and the risk of volume overshooting [9, 15] and recommended close attention to the infant under volume-targeted ventilation [16]. To our knowledge, only one small, unpublished study has yet tested the algorithms of two ventilators on a bench and observed volume overshooting after rapid compliance increase with one ventilator [17]. The aim of this bench study of six modern neonatal ventilators was to assess the adequacy of Vt delivery of their volume-targeted modes when acute resistance, compliance, or leak changes occur, in respect to potential safety issues.
Methods
Test circuit
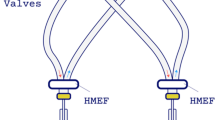
The test circuit was mounted as shown in Fig. 1. The various ventilators equipped with a commercially available standard neonatal respiratory circuit (single-use neonatal respiratory circuit, Fisher & Paykel, Auckland, New Zealand) that allowed rapid leak changes, rapid resistance changes via a Manual Valve Switch (Hans Rudolph, Kansas City, USA) using different airway resistors (Michigan Instruments, Grand Rapids, USA) and rapid compliance changes on the Michigan Infant Training and Test Lung (Model 1601, Michigan Instruments, Grand Rapids, USA). This device simulates an infant respiratory system: the “lung” uses an elastomer bellow and expands as shown in Fig. 1 when gas is inflated via a simulated airway. The compliance can be adjusted from 1 to 15 ml/cmH2O via a lateral spring opposing variable forces against the bellow expansion. The total “lung” capacity is 200 ml and the residual capacity is 70 ml. Expiratory Vt was measured with a Florian Neonatal Respiration Monitor (Acutronic, Hirzel, Switzerland) that has been validated for measurements of very small Vt [18]. The measured data were digitized with a Biopack MP 100 analogue/digital converter (Biopack Systems, Goleta, USA) with 200 samples per second and recorded on a personal computer. The Florian's sensor was located at the Y-piece right before the test lung but after the resistor and leak device and was calibrated according to the user manual before each test series with a new ventilator. The accuracy of its volume measurements was confirmed by the calibrated syringe method prior to our experiences, showing a maximum offset of only 3%.

Test circuit with the ventilator connected to a variable resistor, a variable leak, and a test lung that allowed compliance variations. Respiratory measurements were performed via a Florian Neonatal Respiration Monitor and recorded on a personal computer (PC). P/V-Sensor Pressure/flow sensor. Note: The Servo-i's P/V-Sensor is not located at the Y-piece
Study protocol
Changes in compliance, airway leak, and resistance were systematically introduced and the delivered Vt was recorded. The various ventilators were compared for their effectiveness in maintaining the desired Vt. All experiments were performed simulating full-term and preterm infant settings. Basic full-term infant settings were: Vt 28 ml, resistance 50 cmH2O l−1 s−1, compliance 4 ml/cmH2O, respiratory rate 35 breaths/min, leak 0%, inspiratory time 0.4 s. The following changes were inflicted on the full-term infant system (one parameter change per experiment): (a) compliance change from 4 to 2 ml/cmH2O, from 2 to 6 ml/cmH2O, and stepwise from 2 to 4 to 6 ml/cmH2O, (b) leak change from 30% to 0% and from 0% to 30%, and (c) resistance change from 50 to 200 cmH2O l−1 s−1 and back to 50 cmH2O l−1 s−1 and from 50 to 500 cmH2O l−1 s−1 and back to 50 cmH2O l−1 s−1 (partial obstruction of the endotracheal tube being simulated in the first and its kinking in the second setting). Basic preterm infant settings were: Vt 8 ml, resistance 50 cmH2O l−1 s−1, compliance 2 ml/cmH2O, respiratory rate 50 breaths/min, leak 0%, inspiratory time 0.4 s. The following changes were inflicted on the preterm infant system (one at a time): (a) compliance change from 2 to 1 ml/cmH2O, from 1 to 4 ml/cmH2O and stepwise from 1 to 2 to 4 ml/cmH2O, (b) leak change from 20% to 0% and from 0% to 20%, and (c) resistance change as described above.
In order to isolate the ventilators reaction to any of the above changes only one parameter was changed at a time; all other settings were left at baseline. The compliance and resistance values used were based on lung function testing in healthy and sick infants [19, 20]. All changes were made rapidly from one inflation to the other after observation of a steady state of Vt delivery (generally six inflations in the full-term infant settings and nine inflations in the preterm infant settings were required to achieve this). Only this technique allows us to observe how the ventilators adapt the Vt in response to changes in respiratory mechanics. No further modification were performed during the measurement, neither on the ventilator settings nor in the respiratory system. Vt, PIP, and peak inspiratory flow were recorded for 1 min after each change. Each test series was run five times, and mean values of the measurements were calculated. The standard deviation for delivered Vt was calculated for the five or eight inflations of the steady state before the compliance, resistance, or leak change and for the five or eight final inflations of the measuring period in full-term or preterm infant settings.
The statistical significance of Vt change before and after the inflicted change was tested by one-way analysis of variance for multiple measurements: differences at the level of p < 0.05 were considered to be statistically significant.
Ventilators, modes, and settings
Six modern neonatal ventilators were used, defined by its volume-targeted mode: volume guarantee (Babylog 8000, Dräger Medical, Lübeck, Germany), autoflow (Evita XL, Dräger Medical), adaptive pressure ventilation (Galileo Gold, Hamilton Medical, Rhäzüns, Switzerland), pressure-regulated volume control (Servo-i, Maquet, Solna, Sweden), targeted Vt (SLE 5000, SLE, South Croydon, UK), and volume-assured pressure support (VIP Gold, Bird, Palm Springs, USA; see Table 1). The alarms were set according to the user manual. Where no recommendations were given by the manufacturer, standard alarm settings were used with minimum/maximum Vt alarms at 50%/150% of set Vt, the minimum/maximum minute volume alarm at 50%/150% of the set Vt multiplied with the set respiratory rate, and maximum PIP at 30 cmH2O. In all machines a positive end-expiratory pressure of 5 cmH2O was set.
Following the measurements in volume-targeted mode the entire study protocol was run through with all ventilators set on their conventional pressure-controlled modes. Whenever possible the automatic leak compensation was switched off for the following reasons: (a) not all ventilators offered automatic leak compensation, or (b) pilot measurements with automatic leak compensation showed inconsistent breath-to-breath variation in Vt delivery and PIP.
Results
Compliance decrease
Considerable discrepancies between the set Vt and the delivered volumes were observed under prechange conditions (Vt ranged from 68% to 147% of the set value; Fig. 2, Table 2). All ventilators showed volume undershooting after lowering the compliance, at least during some inflations, under full-term infant settings. The machines varied in the extent of volume undershooting, the number of inflation before reaching a steady state and its adequacy compared to the set Vt value. Compliance decrease was well managed by all machines under preterm infant settings without major changes in delivered Vt compared to baseline conditions. Two ventilators showed a cyclic instability of the delivered Vt: the Evita XL showed breath-to-breath variation after the change (full-term infant settings) and under prechange conditions (preterm infant settings), whereas the Galileo Gold showed a sinusoidal pattern of Vt delivery without achieving a new steady state after the change (full-term infant settings). The VIP Gold and SLE 5000 did not adjust their Vt after the compliance change.

Compliance decrease from 4 to 2 ml/cmH2O (2 to 1 ml/cmH2O) in a full-term and b preterm infant settings. V t Tidal volume; horizontal solid bar set Vt of 28 ml (8 ml) in full-term (preterm) infant settings; horizontal dotted bar set Vt of 25 ml (10 ml) for Galileo Gold (Galileo Gold and VIP Gold) ventilator in full-term (preterm) infant settings; vertical bar compliance change before inflation number six (nine) in full-term (preterm) infant settings; filled circles Babylog 8000 plus; filled squares Evita XL; filled triangles Galileo Gold; open circles Servo-i; open squares SLE 5000; open triangles VIP Gold
Compliance increase
All ventilators showed volume overshooting above the set value, although to variable extent (Fig. 3, Table 2). The ratio between the maximally delivered volume and the set Vt was consistently higher in the low Vt range: under full-term infant settings (compliance change from 2 to 6 ml/cmH2O) this overshooting ranged from 130% of set Vt (Babylog 8000+, Evita XL, Servo-i) to 163% (Galileo Gold), whereas under preterm infant settings (compliance change from 1 to 4 ml/cmH2O) it ranged from 115% (VIP Gold) to 234% (Galileo Gold). Between one and 13 inflations were needed for the various machines to achieve a new steady state. The Servo-i, however, overshot only once and then lowered the delivered volume significantly for the following inflation before approaching the new steady state by small Vt increments from one inflation to the other. The Evita XL showed again breath-to-breath variability under prechange full-term infant settings, and the VIP Gold as well as the SLE 5000 showed only minimal Vt adjustment after the change. The same pattern of volume overshooting was observed (although to a lesser extent) when the compliance was increased stepwise (data not shown).

Compliance increase from 2 to 6 ml/cmH2O (1 to 4 ml/cmH2O) in a full-term and b preterm infant settings. V t Tidal volume; horizontal solid bar: set Vt of 28 ml (8 ml) in full-term (preterm) infant settings; horizontal dotted bar set Vt of 25 ml (10 ml) for Galileo Gold (Galileo Gold and VIP Gold) ventilator in full-term (preterm) infant settings; vertical bar compliance change before inflation number six (nine) in full-term (preterm) infant settings; filled circles Babylog 8000 plus; filled squares Evita XL; filled triangles Galileo Gold; open circles Servo-i; open squares SLE 5000; open triangles VIP Gold
Leak changes
Leak increase or decrease was generally well managed by most ventilators, and we observed only minor variations in Vt delivery. For a more detailed description of theses results see Electronic Supplementary Material (ESM; Fig. 1, 2, Table 1).
Resistance increase
All ventilators dropped their Vt for the first inflations after the resistance increase (Fig. 4 and Table 3 show results of the 50 to 200 cmH2O l−1 s−1 increase; for data on the 50 to 500 cmH2O l−1 s−1 increase see ESM). This drop was less pronounced with the lower set Vt (minimal volume 45–50% under full-term infant settings for the majority of machines and 65–87% under preterm infant settings). Most ventilators adapted the delivered volume to prechange level within 3–14 inflations. The VIP Gold showed only minor Vt variation whereas the SLE did not adapt its volume to the new condition. Under preterm infant settings the Evita XL again demonstrated the described breath-to-breath Vt variability, before and after the change.

Resistance increase from 50 to 200 cmH2O l−1 s−1 in a full-term and b preterm infant settings. V t Tidal volume; horizontal solid bar set Vt of 28 ml (8 ml) in full-term (preterm) infant settings; horizontal dotted bar set Vt of 25 ml (10 ml) for Galileo Gold (Galileo Gold and VIP Gold) ventilator in full-term (preterm) infant settings; vertical bar compliance change before inflation number six (nine) in full-term (preterm) infant settings; filled circles Babylog 8000 plus; filled squares Evita XL; filled triangles Galileo Gold; open circles Servo-i; open squares SLE 5000; open triangles VIP Gold
Resistance decrease
All ventilators delivered lower than set Vt under high resistance conditions in full-term infant settings, whereas the Vt was more adequately achieved in preterm infant settings (Fig. 5 and Table 3 show results of the 200 to 50 cmH2O l−1 s−1 increase; for data on the 500 to 50 cmH2O l−1 s−1 increase see ESM). All machines except the VIP Gold overshot the delivered volume above the set value in full-term infant settings, with a maximal volumes ranging from 119% of the set value (Servo-i) to 173% (Galileo Gold). The Servo-i behaved in the same way as after the compliance increase and administered only one inflation above the set value, lowered significantly the delivered Vt for the following inflation before approaching a steady state close to the set value by small breath-to-breath volume increments. Under preterm infant settings the delivered volume of all ventilators increased after resistance decrease but to a lesser extent than under full-term infant settings. The Evita XL, however, again showed the described breath-to-breath variability, the Servo-i delivered Vt well below the set value before and after the change, and the Galileo Gold started a sinusoidal pattern of volume delivery with the resistance decrease (Vt between 7 and 10 ml; set value 10 ml). There was of course no volume adaptation in any of the pressure-control modes in any of the above settings (data not shown).

Resistance decrease from 200 to 50 cmH2O l−1 s−1 in a full-term and b preterm infant settings. V t Tidal volume; horizontal solid bar set Vt of 28 ml (8 ml) in full-term (preterm) infant settings; horizontal dotted bar set Vt of 25 ml (10 ml) for Galileo Gold (Galileo Gold and VIP Gold) ventilator in full-term (preterm) infant settings; vertical bar compliance change before inflation number six (nine) in full-term (preterm) infant settings; filled circles Babylog 8000 plus; filled squares Evita XL; filled triangles Galileo Gold; open circles Servo-i; open squares SLE 5000; open triangles VIP Gold
Discussion
Published data on the stability of Vt delivery during volume-targeted ventilation are conflicting [6, 7, 12, 14, 17]. The aim of this study was to evaluate how the ventilators algorithms manage to stabilize the delivered Vt after deliberately rapid modifications in respiratory mechanics. The most important observation was that important volume overshooting occurred in all ventilators after compliance increase and resistance decrease (Figs. 3, 5; Tables 2, 3). The difference between the tested machines can be found in the degree of volume overshooting, the response time needed to bring the Vt back to baseline, the ability to achieve a steady state at the set value, and the way in which these changes were handled by the built-in algorithm. The most alarming observations were made under “preterm infant” test conditions (i. e., set Vt of 8 and 10 ml, respectively). After compliance increase one ventilator overshot the Vt up to 234% of set value and others up to 190%. Only the Evita XL, Servo-i, and VIP Gold kept their Vt within the 150% range, which might be considered to be acceptable in the clinical setting. The Evita XL, VIP Gold, and SLE 5000 behaved as in a pressure-control mode, without lowering Vt towards the set value after the initial overshot; the Galileo Gold and Babylog 8000 plus needed 7–11 inflations to reach steady state again at acceptable Vt. The Servo-i had the quickest response time and showed a unique particularity in its algorithm. Delivered Vt is lowered dramatically after the first overshoot inflation; there was then a trend in Vt values toward baseline by small volume adjustments. This is a very safe way to react to volume overshooting. Most other machines delivered too high Vt after these changes. The same pattern can be observed in “full-term infant” conditions (i. e., set Vt of 28 or 25 ml) after compliance increase. Under this condition only the Galileo Gold and SLE 5000 showed more than 150% volume overshooting. Vt after resistance decrease increased to 182% (Galileo Gold) of set values, but most ventilators did not overshoot to more than 40 ml. Our results are consistent with the findings of an unpublished bench study comparing the Babylog 8000 plus with the VIP Gold that observed variable volume overshooting as well [17].
The lower than set Vt delivery was transient with most ventilators after compliance decrease and resistance increase in preterm and full-term infant settings (Figs. 2, 4; Tables 2, 3). However, the transient tendency to deliver lower than set Vt is of less clinical concern. The final adaptation of Vt in volume-targeted modes can be pointed out as a clear advantage over conventional pressure control modes since the latter continues to deliver a low Vt until the operator adjusts the PIP manually. Leak changes (up or downwards) were generally well handled by all ventilators, and only minor changes in Vt delivery were noted (see ESM, Figs. 1, 2, Table 1).
With some settings considerable Vt discrepancy from the set value was observed after the inflected change but even under baseline conditions. This may be due to any of several factors, including a flow sensor not located at the Y-piece (as in the Servo-i) and differences in flow algorithms applied. Under low compliance and high resistance settings the inadequate Vt delivery may be due to the discrepancy of the respiratory system's time constant and the set inspiratory time of 0.4 s. This hypothesis is supported by the absence of a high PIP alarm in most ventilators. We chose this inspiratory time as it is a classical setting in many neonatal care units, and we elected not to adapt this setting after the changes as this rarely happens in daily practice.
Some ventilators showed considerable variation in delivered Vt, which seems to be a result of the volume adjustment algorithm used. The Evita XL showed a breath-to-breath variability of ± 25% around the set value. This variability was abolished or attenuated under high resistance and low compliance settings. This may be due to the fact that the Evita XL's algorithm adjusts PIP by steps of 3 cmH2O in order to match the expiratory Vt with the set value. In conditions with low resistance and high compliance this leads to a falsely high volume, which triggers the feedback decrease in PIP that leads to a Vt lower than the target volume and so on. The Galileo Gold showed a sinusoidal pattern of Vt delivery after compliance decrease (set Vt of 28 ml), leak changes (set Vt of 10 ml) and resistance decrease (set Vt of 10 ml), which may be due to the fact that its algorithm targets the set Vt over a longer period of time by progressive PIP increases or decreases.
There are differences in the way in which the various ventilators target the Vt. The details of the algorithms are part of the manufacturers art to build respirators and they are therefore not available for all machines (Table 1). These vary substantially between the various machines tested in this study. It would be helpful for the clinician to have easy access to the ventilator algorithms in detail in order to decide whether a specific patient can be considered eligible for this ventilation mode and to take appropriate bedside decisions. Short-term ventilation with high Vt has been clearly shown to be detrimental to the patients lung [21]. Large Vt (certainly if higher than 9 ml/kg) can lead to overdistension [22] and increased incidence of acute lung injury [23]. However, there is to our knowledge no evidence concerning the adverse effect of acute application of high Vt (if not excessive [24]) for only a few inflations and no critical threshold can therefore be determined above which lung injury may be worsened. The settings chosen in our study may not reflect clinical situations completely; some changes were more rapid and some of them extremer than those commonly encountered at the bedside. However, these artificial events allowed us to isolate the exact way the various ventilator algorithms deal with changes in respiratory mechanics and help us to better understand the patient–ventilator interaction in this relatively new ventilation mode. In addition, we believe that the extent of volume overshooting that we observed under some circumstances can be of clinical concern, even if the high Vt is applied for only a short period of time.
In conclusion, using volume-targeted mode some ventilators showed important Vt overshooting upon rapid changes in respiratory mechanics (i. e., compliance increase or resistance decrease) that may be of clinical concern. Some ventilators did not achieve the set Vt after compliance decrease or resistance increase, which may lead to inadvertent hypoventilation. Therefore clinical studies are needed to determine the significance of our observations from the bench to determine complication rate and patient outcome with this relatively new ventilator mode. We also encourage manufacturers to further improve their ventilator algorithms governing volume delivery in volume-targeted modes.
References
Clark RH, Gerstmann DR, Jobe AH, Moffitt ST, Slutsky AS, Yoder BA (2001) Lung injury in neonates: causes, strategies for prevention, and long-term consequences. J Pediatr 139:478–486
Chiumello D, Pristine G, Slutsky AS (1999) Mechanical ventilation affects local and systemic cytokines in an animal model of acute respiratory distress syndrome. Am J Respir Crit Care Med 160:109–116
Network TARDS (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 342:1301–1308
Keszler M (2005) Volume-targeted ventilation. J Perinatol (Suppl 2) 25:S19–S22
Lista G, Marangione P, Azzali A, Castoldi F, Pogliani L, Compagnoni G (2000) [The “guaranteed volume” in pressure support ventilation reduces the risk of barotrauma in premature children with severe respiratory syndrome]. Acta Biomed Ateneo Parmense (Suppl 1) 71:453–456
Abubakar KM, Keszler M (2001) Patient-ventilator interactions in new modes of patient-triggered ventilation. Pediatr Pulmonol 32:71–75
Lista G, Colnaghi M, Castoldi F, Condo V, Reali R, Compagnoni G, Mosca F (2004) Impact of targeted-volume ventilation on lung inflammatory response in preterm infants with respiratory distress syndrome (RDS). Pediatr Pulmonol 37:510–514
Herrera CM, Gerhardt T, Claure N, Everett R, Musante G, Thomas C, Bancalari E (2002) Effects of volume-guaranteed synchronized intermittent mandatory ventilation in preterm infants recovering from respiratory failure. Pediatrics 110:529–533
Keszler M, Abubakar K (2004) Volume guarantee: stability of tidal volume and incidence of hypocarbia. Pediatr Pulmonol 38:240–245
Mrozek JD, Bendel-Stenzel EM, Meyers PA, Bing DR, Connett JE, Mammel MC (2000) Randomized controlled trial of volume-targeted synchronized ventilation and conventional intermittent mandatory ventilation following initial exogenous surfactant therapy. Pediatr Pulmonol 29:11–18
Sinha SK, Donn SM, Gavey J, McCarty M (1997) Randomised trial of volume controlled versus time cycled, pressure limited ventilation in preterm infants with respiratory distress syndrome. Arch Dis Child Fetal Neonatal Ed 77:F202–205
Piotrowski A, Sobala W, Kawczynski P (1997) Patient-initiated, pressure-regulated, volume-controlled ventilation compared with intermittent mandatory ventilation in neonates: a prospective, randomised study. Intensive Care Med 23:975–981
Cheema IU, Ahluwalia JS (2001) Feasibility of tidal volume-guided ventilation in newborn infants: a randomized, crossover trial using the volume guarantee modality. Pediatrics 107:1323–1328
Lista G, Colnaghi M, Castoldi F, Fontana P, Reali R, Mosca F, Compagnoni G (2003) [Lung injury and ventilatory strategies]. Pediatr Med Chir 25:35–41
McCallion N, Davis PG, Morley CJ (2004) Volume-targeted versus pressure-limited ventilation in the neonate. Cochrane Database of Systematic Reviews, Cochrane Library
Riley C, Pilcher J (2003) Volume-guaranteed ventilation. Neonatal Netw 22:17–22
Collins E, Faciane V, Abbruzzese L (2005) Comparison of Bird Vip Gold ventilator in conventional volume mode to Drager Babylog 8000 Plus in volume guarantee mode a bench study. http://www.viasyshealthcare.com/prod_serv/downloads/045_Volume_Accuracy_Monograph.pdf; accessed 18 September
Scalfaro P, Pillow JJ, Sly PD, Cotting J (2001) Reliable tidal volume estimates at the airway opening with an infant monitor during high-frequency oscillatory ventilation. Crit Care Med 29:1925–1930
Hjalmarson O, Sandberg K (2002) Abnormal lung function in healthy preterm infants. Am J Respir Crit Care Med 165:83–87
Kavvadia V, Greenough A, Itakura Y, Dimitriou G (1999) Neonatal lung function in very immature infants with and without RDS. J Perinat Med 27:382–387
Dreyfuss D, Saumon G (1998) Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med 157:294–323
Roupie E, Dambrosio M, Servillo G, Mentec H, el Atrous S, Beydon L, Brun-Buisson C, Lemaire F, Brochard L (1995) Titration of tidal volume and induced hypercapnia in acute respiratory distress syndrome. Am J Respir Crit Care Med 152:121–128
Gajic O, Dara SI, Mendez JL, Adesanya AO, Festic E, Caples SM, Rana R, St Sauver JL, Lymp JF, Afessa B, Hubmayr RD (2004) Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med 32:1817–1824
Bjorklund LJ, Ingimarsson J, Curstedt T, John J, Robertson B, Werner O, Vilstrup CT (1997) Manual ventilation with a few large breaths at birth compromises the therapeutic effect of subsequent surfactant replacement in immature lambs. Pediatr Res 42:348–355
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Jaecklin, T., Morel, D.R. & Rimensberger, P.C. Volume-targeted modes of modern neonatal ventilators: how stable is the delivered tidal volume?. Intensive Care Med 33, 326–335 (2007). https://doi.org/10.1007/s00134-006-0450-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0450-9