Article Text

Abstract
Objective Malawi has the highest estimated preterm birth rate in the world. The survival rate of these babies is not known. The main objective of this study was to demonstrate the short-term survival of infants with birth weight below 2500 g nursed in Bwaila Hospital, a district hospital, and the tertiary level Kamuzu Central Hospital (KCH) in Lilongwe. The specific objectives were to calculate birth weight specific survival rates, compare the two hospitals regarding the chances of survival and review the use of antenatal corticosteroids.
Design 1496 babies were included prospectively in the study between June and November 2012. Survival was defined as discharge from the nursery or postnatal ward.
Results Survival was 7% for extremely low birth weight infants, 52% for very low birth weight and 90% for low birth weight (1500–2499 g). There was a marked increase in survival from 1100 g. Survival was significantly higher in KCH only for babies weighing below 1200 g. The majority of deaths occurred within the first 3 days of life. Only 98 of the babies had a mother who had received antenatal corticosteroids.
Conclusions With the current resources, we suggest focusing efforts on preventing early neonatal deaths in low birth weight infants above 1100 g in the hospitals in Lilongwe. The coverage of antenatal steroids for mothers at risk of preterm delivery can be improved. Further studies are needed on the quality of the obstetric and neonatal care at the hospitals and how to reduce the high rate of preterm birth in Malawi.
- Premature
- low birth weight
- survival
- mortality
- neonatology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
What is already known on this topic?
-
Every year, over a million babies die due to prematurity, which is now the second most common cause of death in children under five.
-
Malawi had the highest estimated preterm birth rate in the world in 2010.
-
Antenatal corticosteroids decrease the risk of mortality in premature infants.
What this study adds?
-
Survival was 7% for extremely low birth weight infants, 52% for very low birth weight and 90% for low birth weight (LBW) (1500–2499 g).
-
The main focus should be to improve the care of the heavier LBW infants.
-
The use of antenatal corticosteroids is very low in Malawi. Increased coverage of antenatal corticosteroids could save lives.
Introduction
Every year, an estimated 14.9 million babies are born preterm worldwide.1 Over a million of these babies die due to complications of preterm birth, which is now the second most common cause of death after pneumonia in children under 5 years old.2 In 2010, the global average preterm birth rate was 11.1%. The same study showed that Malawi had the highest preterm birth rate in the world, estimated to be 18%.1 The rate of neonatal survival of these babies has previously not been investigated.
Malawi is one of the poorest countries in the world with a gross national income per capita of less than US$1/day, the maternal mortality ratio is among the highest in the world, the neonatal mortality rate was 31/1000 and the under-five mortality was 112/1000 live births in 2010.3–5 In clinical practice, the gestational age is often uncertain, whereas the birth weight is more likely to be known if born in a health facility. WHO defines low birth weight (LBW), a result of preterm birth and/or intrauterine growth restriction, as birth weight less than 2500 g.6 An estimated 12%–15% of the 600 000 babies born each year in Malawi are LBW.3 ,7
The main objective of this study was to demonstrate the short-term survival of infants with LBW nursed in Bwaila Hospital (BH) and Kamuzu Central Hospital (KCH) in Lilongwe, Malawi. The specific objectives were to calculate birth weight specific survival rates, compare the two hospitals regarding the chances of survival for LBW infants and review the use of antenatal corticosteroids.
Method
In Lilongwe, the capital of Malawi, there are two public hospitals: the tertiary level KCH and BH, a district hospital. The hospitals are situated 4 km apart. Sick infants are referred to these nurseries from health facilities in the entire central region with a population of 4 million people. KCH receives the sickest high-risk obstetric patients from the same area, including BH. Annually, KCH conducts approximately 3000 and BH 14 000 deliveries and their nurseries admit approximately 1000 and 4800 babies, respectively. BH is mainly run by midwives/nurses, clinical officers and non-specialised doctors. In KCH, there are in addition a small number of specialist-trained doctors in the obstetric and paediatric departments. Neither of the hospitals routinely uses tocolytics to prevent preterm delivery and the availability of antenatal corticosteroids and antibiotics is erratic. The nurseries have oxygen, heaters, intravenous fluids, aminophylline and antibiotics. Kangaroo Mother Care (KMC) with skin-to-skin contact, exclusive, early breast feeding, early discharge and close follow-up are the standard care for stabilised infants in the nurseries.8 However, KMC is seldom started in the labour wards and as most babies are kept in cot beds for the first few days, the establishment of the skin-to-skin contact is often delayed. One very simple continuous positive airway pressure (CPAP) machine is available in KCH. Mechanical ventilation and surfactant are not available. At present, there are no official guidelines between the two nurseries regarding the specific birth weight at which babies should be referred from BH to KCH.
This was mainly a prospective descriptive study of the survival of live born infants with birth weights below 2500 g, nursed in KCH and BH during the time period of 1 June–30 November 2012. The babies born in June were studied retrospectively. Included were babies that were either admitted to the nurseries (including babies with birth places other than KCH and BH), those born alive but who died in the labour wards of KCH and BH and those nursed with their mothers in the postnatal wards. Survival was defined as alive on discharge from the nursery or postnatal ward. Excluded were babies with severe congenital malformations, birth weight of less than 600 g (the cut-off between miscarriages and premature deliveries in Malawi is 28 gestational weeks—the 3rd percentile of weight at 28 weeks is approximately 600 g)9 and babies with unknown outcome. Babies born outside of KCH and BH were included if their age was less than 48 h on admission, as other factors such as care by traditional healers and malpractice in other hospitals could affect the outcome. The data were collected from the maternity registers, nursery admission books, duty report books and all available obstetric case records. In KCH, all neonatal case records were used whereas in BH the neonatal case records were obtained only in cases with unclear outcome. The data were entered in an Excel worksheet. SAS Enterprise Guide 5.1 was used for descriptive statistical analysis and Fisher exact test was performed with α=0.05. According to the WHO definition, LBW was further subdivided into very low birth weight (VLBW) (1000–1499 g) and extremely low birth weight (ELBW) (<1000 g).6 The study was approved by the College of Medicine Research and Ethics Committee, Blantyre, Malawi.
Results
In this study, 1496 babies were included after exclusion of 56 babies (34 babies due to unknown outcome, nine due to birth weight less than 600 g, seven due to severe malformations and six babies born outside BH and KCH due to an age >48 h on admission). Two babies with cleft palate and one baby with clubfeet were included in the study, as those deformities were not considered fatal. A total of 1101 babies were nursed in BH and 395 in KCH. Overall, 1289 mothers gave birth to the 1496 babies (table 1).
Maternal characteristics
KCH had a higher proportion of ELBW and VLBW babies (table 2). In all, 64 babies were referred from the nursery in BH to KCH; these babies are presented as belonging to KCH in the following presentation.
Characteristics of infants
Of those with known birthplace, 92% were born in a health facility. Overall, 52% of the babies were girls and 48% boys. In both hospitals, 66% of the babies were singleton, 32% twins and 2% triplets or more. The percentage of babies born via caesarean section (CS) was significantly higher in KCH (30%) than in BH (15%, p<0.001). More babies in KCH than in BH had a mother with hypertensive disorder (35% vs 9%; p<0.001).
The survival was 7% for the ELBW infants, 52% for VLBW and 90% for LBW (1500–2499 g). Due to the higher proportion of heavier babies in BH, the overall survival was higher in BH than KCH (p=0.002) (table 3). Very few babies below 1100 g survived but at 1100 g there was a marked increase in survival (figure 1). The data suggest that the survival for ELBW and VLBW was higher in KCH than in BH; however, the difference was only statistically significant for babies below 1200 g (p=0.002) (figure 2). For infants weighing above 2000 g, the survival was higher in BH than in KCH (p=0.015). There was no significant difference in survival depending on mode of delivery.
Survival per birth weight category
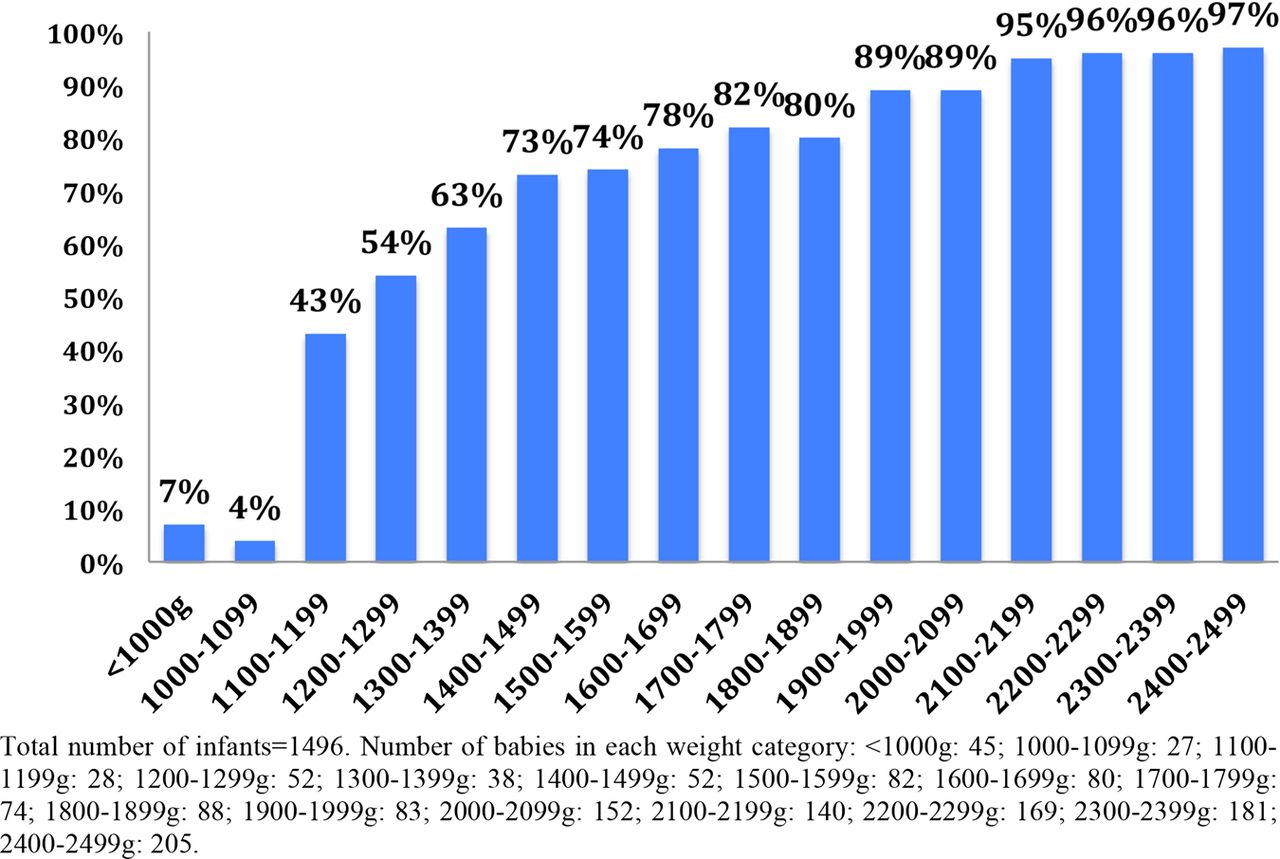
Survival rates per birth weight category.

{kind=link}
{kind=link}
Survival rates of extremely low birth weight and very low birth weight per Bwaila Hospital (BH) and Kamuzu Central Hospital (KCH).
A majority (82%) of deaths occurred within the first 3 days of life. In BH, 40% of the babies died within their first 24 h of life, compared with 16% in KCH (table 4).
Age at death
In total, 98 babies were known to have a mother who had received some antenatal corticosteroids (out of 1010 with known information about antenatal corticosteroids). However, only 34 of those babies had been exposed to a full course of four doses of 6 mg dexamethasone 12 hourly. In all, 59 were nursed in KCH and 39 in BH. The coverage of antenatal steroids was higher in KCH (24%) than in BH (5%) (p<0.001). The survival was 85% for babies exposed to steroids (average weight was 1821 g) and 83% without steroids (average weight 1923 g). Overall, 42 babies in KCH were treated with CPAP; out of these, 35 died.
Discussion
In the present study on neonatal mortality among LBW infants in two big Malawian hospitals, we found an overall neonatal mortality rate of 17%, reaching 48% and 93% in the groups of neonates with birth weights 1000–1499 g and <1000 g, respectively. For babies <1200 g only, neonatal survival was higher in the tertiary hospital with better personnel and equipment resources. Most deaths occurred within the first 3 days of life. The coverage of antenatal steroids was less than 10%. A small minority of newborns were treated with CPAP, in most cases without any positive effect.
Few studies have been made on the survival of LBW in similar settings in other low-income countries. Studies published in the 1990s showed similar rates of survival in Ghana and Nigeria with survival of ELBW of 10%–17%, of VLBW of 47% and LBW of 89%.10 ,11 Newer reports from less resource poor settings, but without access to surfactant and ventilators, show survival of up to 30% for ELBW, 67%–83% for VLBW and 98% for LBW.12 ,13 Hence there is room for improvement in KCH and BH.
Most babies below 1000 g need neonatal intensive care to survive.14 As there are no neonatal ventilators and no surfactant available in BH or KCH, the poor outcome of the ELBW babies was expected.
Even though the survival rate increased with increasing weight, in numbers, equally as many babies below as above 1500 g died in this study. A majority of deaths occurred within the first 3 days of life. The most common causes of death within the first few days of life in preterm infants are asphyxia, hypothermia, hypoglycaemia, neonatal sepsis and respiratory distress syndrome (RDS).15 The majority of these conditions can be treated or prevented with relatively simple means by resuscitation, early and continuous skin-to-skin contact to prevent hypothermia, improved early-feeding practices to prevent hypoglycaemia, antibiotics to treat infections and antenatal corticosteroids, oxygen and access to simple CPAP treatment to prevent and treat RDS.8 ,15–17 Improvement in these areas would likely improve the survival of the heavier babies significantly. As 40% of the deaths in BH happened within the first day (compared with 16% in KCH), special efforts should be put into improving resuscitation measures in BH. In both hospitals, the KMC and the early feeding are often delayed by a practise of wrapping the baby in cloths and putting it aside after successful resuscitation. Sometimes, this is due to complications of the mother that need to be dealt with and not enough staff. However, most mothers have an accompanying guardian who could give skin-to-skin contact already in labour ward and take the baby to the nursery for feeds and further care within the first hour.
As almost all CPAP treated babies in this study died, the use of the CPAP machine and the timing of initiating CPAP treatment need to be revised. As the machine is not used on a daily basis and there is a high turnover of staff, there might be improvement by offering training for the staff on a regular basis. Given the limited resources in BH and KCH and the high risk of sequelae for the smallest babies, this study suggests that efforts should currently be focused on the infants with a birth weight of more than 1100 g (figure 1).14 ,18
KCH had, as the tertiary hospital, a higher proportion of ELBW and VLBW, resulting in a higher overall mortality rate. Despite the fact that KCH received many of the smallest and sickest babies from BH and other facilities as referrals, the survival was equal or better than in BH for babies below 2000 g. Access to paediatricians, better equipment and more nursing staff per baby in KCH might have contributed to the better outcome. One could also argue that a baby that survived the transfer to KCH, which sometimes can take hours from some of the district hospitals, has somehow already proven to be strong.
There are currently no guidelines agreed upon for referrals of babies with LBW between the two hospitals in Lilongwe. If the tertiary level hospital had enough resources in terms of beds, staff and supplies, it would probably be wise to centralise the care of all infants below 1500 g. Ultimately, those babies should be transferred in utero. However, with the current limited resources and the very poor outcome for infants below 1100 g, we suggest referral of babies weighing 1100–1200 g to the tertiary level.
The CS rate of 18% is higher than the 5%–15% recommended by WHO and may have affected the survival of the babies (table 1).19 The national rate of CS is 4.6%.3 The high rate of CS in the central hospitals reflects the poor health status of these mothers and the high percentage of multiple gestations. In each case of provider initiated delivery and CS, the obstetrician must balance the mother's condition with the risks that prematurity mean to the baby and surgery to the mother.
Antenatal corticosteroids significantly reduce neonatal morbidity, mortality and need for respiratory support in preterm infants.20 Surprisingly, this study did not support any conclusions on the efficiency of antenatal corticosteroids. However, the numbers were very small, the average weight of the exposed babies was slightly lower than of the non-exposed and few of the exposed babies had a full course (and therefore the full benefit) of the antenatal corticosteroids. Many mothers were admitted when in active labour and delivered shortly after admission. As a tertiary centre, KCH had a higher proportion of mothers who were admitted due to complications of pregnancy, for example, preeclampsia. The longer admission times prior to delivery for the sick mothers in KCH may have allowed time for administration of antenatal corticosteroids, but their disease might also have added to the risk of morbidity and mortality of their babies.
In this study, less than 10% of the babies had a mother who had received antenatal corticosteroids and only 4% had had a full course. The coverage was lowered by the fact that during the study period, corticosteroids were intermittently unavailable in the pharmacies of the two hospitals. The availability and use of antenatal corticosteroids need to increase. Possibly the coverage would increase if injectable corticosteroids are stocked in health centres and district hospitals, where mothers at risk of preterm delivery could be treated before referral to the maternity units.
From an obstetric point of view, persistent malaria, maternal undernourishment and anaemia have been associated with preterm birth in Malawi.21 More research is needed to investigate the causes of premature birth and LBW and why Malawi has such high rates of especially preterm birth. Improved quality of the components of the antenatal clinics and focus on risk factors for preterm birth could possibly help to identify the mothers at risk and enable referral to the most adequate level of care for them.
We acknowledge some weaknesses of the present study. The study was conducted in the two hospitals in the capital city, which have a higher standard of care than most other hospitals in the country, and hence the findings cannot be generalised for all of Malawi. The preterm birth rate could not be calculated in this study, as both inborn and outborn babies were included. We only investigated the short-term survival of the infants with LBW. We have no information on the causes of death or the long-term survival or morbidity, which in many cases might be lifelong and be a heavy burden on the individuals, the families and health systems.18 ,22 These issues need to be addressed to reduce the under-five mortality in Malawi.
Acknowledgments
Thanks to: Professor J Sundby, Dr D Wackernagel and Dr H Nisell for medical, scientific and editorial advice, Dr G Chiudzu and the staff at BH and KCH for general support. We especially thank the late Mr Michael Mponda who helped in collecting the medical files; without his devotion to work for better statistics to improve maternal health in Malawi, this study would not have been possible to conduct.
References
Footnotes
-
Contributors AKA designed the study, obtained the Ethics Committee approval, collected data and wrote the manuscript draft and revised it. ES contributed to the design of the study, performed the statistical analyses and critically reviewed the draft. NK collected data and critically reviewed the draft of the study. FK contributed to the design of the study and reviewed the draft. KW contributed to the design and reviewed the draft. All authors approved of the final version of the manuscript and agreed to be accountable for the work.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval This study was approved by the College of Medicine Research and Ethics Commitee, Blantyre, Malawi.
-
Provenance and peer review Not commissioned; externally peer reviewed.