Article Text

Statistics from Altmetric.com
This female infant was born at 34 weeks of gestation by spontaneous vaginal delivery following increasing polyhydramnios and premature rupture of membranes. At 22 weeks of gestation, a left-sided diaphragmatic hernia with minimal mediastinal shift and a favourable head-to-lung ratio had been diagnosed. After delivery, following a short period of bag-mask ventilation with apparently appropriate chest excursions, oro-tracheal intubation was performed without difficulty by a senior neonatologist. When no chest excursions were visible despite high inspiratory pressures, endotracheal tube malposition was assumed and bag-mask ventilation was restarted. Although chest movements were again noted, the infant's heart rate and transcutaneous oxygen saturation did not improve. Additional intubation and ventilation attempts remained unsuccessful, and the infant died despite extended resuscitation efforts.
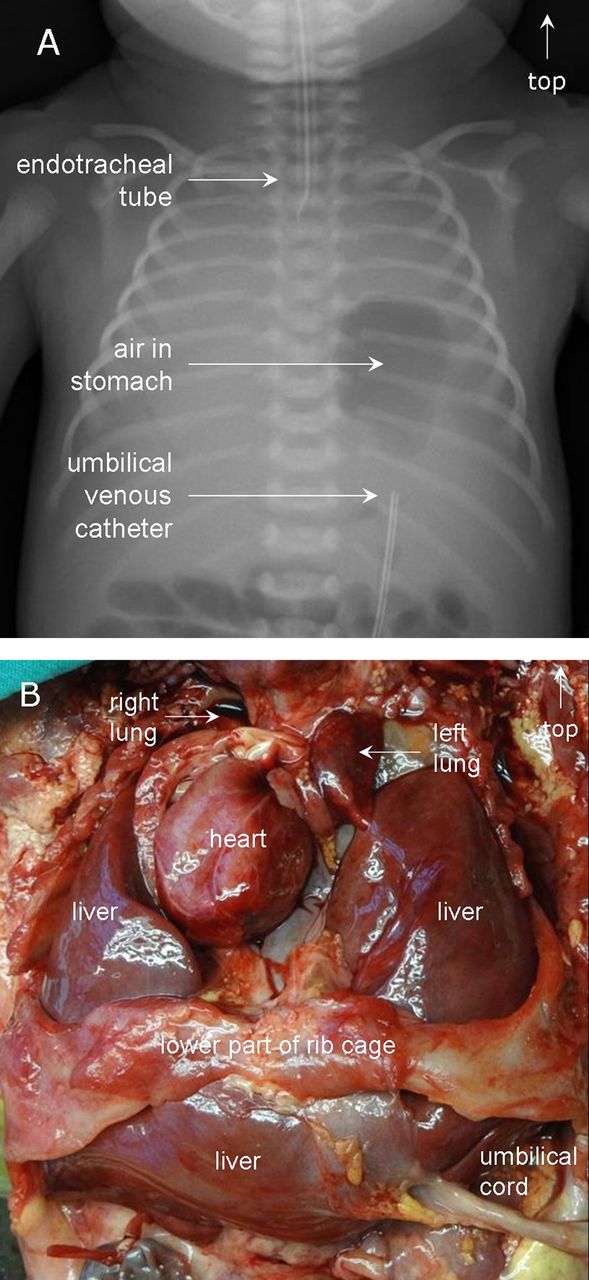
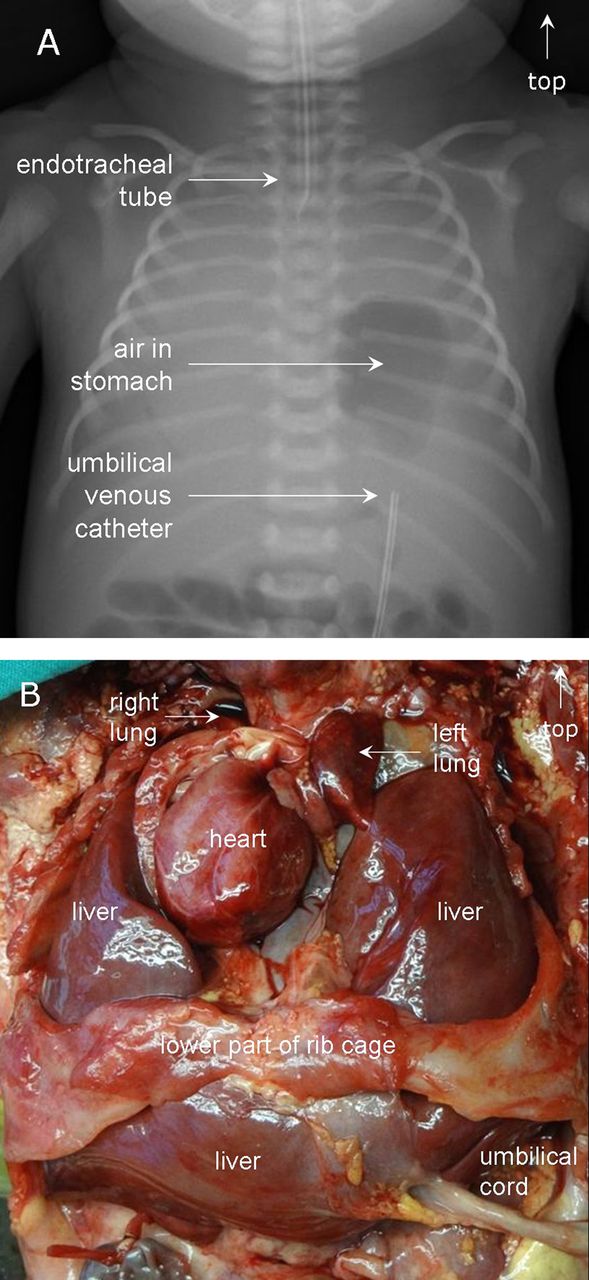
Because chest excursions were noted during bag-mask ventilation, but absent when ventilation was attempted through an endotracheal tube, tracheal agenesis with oesophago-tracheal fistula was suspected. However, a postmortem chest x-ray showed air in the herniated stomach but no lung aeration (figure 1A), and at autopsy, bilateral diaphragmatic agenesis with u-shaped liver herniation and severe pulmonary hypoplasia incompatible with life were demonstrated (figure 1B). In addition, there was a cloacal malformation. Apparently, the herniated liver had been misinterpreted as lung tissue on prenatal ultrasound examination because of comparable echodensity of liver and fluid-filled fetal lungs. The lack of a significant mediastinal shift was felt to support the impression of a small hernia, but obviously was due to bilateral herniation.
{kind=link}
(A) Postmortem chest radiograph showing complete absence of lung aeration; (B) Autopsy demonstrating bilateral herniation of liver lobes and severe pulmonary hypoplasia.
The autopsy findings in our patient fully explained the observations made during resuscitation and clarified why resuscitation was doomed to fail. This information was of utmost importance both to the parents as well as the members of the resuscitation team.
Footnotes
-
Contributors The manuscript draft and the figures were prepared by the first author (TMB); the second author (MJ) reviewed the manuscript and made suggestions for improvements. Both authors approved of the final manuscript. The first author (TMB) is responsible for the overall content as guarantor.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.