Article Text

Abstract
Background: During volume guarantee (VG) ventilation the peak inflating pressure (PIP) for each ventilator inflation is adjusted to ensure the expired tidal volume (VTe) is close to the set VTe. Differences in the PIP between inflations triggered by the infant’s inspirations and untriggered inflations are seen.
Aim: To investigate the effects of triggered and untriggered inflations on PIP and VTe.
Methods: Neonates were ventilated with the Dräger Babylog 8000 using assist control (synchronous intermittent positive pressure ventilation) and VG modes. Continuous recordings of ventilator pressures and tidal volumes were made at 200 Hz for 10 minutes.
Results: In 10 infants, 6540 inflations were analysed, of which 4052 (62%) were triggered. Triggered inflations had a significantly lower mean (SD) PIP than untriggered inflations: 12.9 (4.9) vs 17.0 (3.3) cm H2O, (p<0.001). Despite this, there was no significant difference in the VTe of each type of inflation (103% and 101% of the set VTe, respectively). When a triggered inflation was immediately preceded or followed by an untriggered inflation the PIP changed by about 5 cm H2O. Between adjacent inflations of the same type, the change in PIP was less than 3 cm H2O: for triggered inflations it was 0.11 (1.50) cm H2O and for untriggered inflations 0.06 (1.53) cm H2O.
Conclusion: During VG ventilation with the Dräger Babylog 8000 the PIP was 4 cm H2O lower during triggered inflations than untriggered inflations, although the expired tidal volumes were similar.
Statistics from Altmetric.com
Increased awareness of the role of volutrauma, and lung overdistension in the pathogenesis of ventilator-induced lung injury in animal models and adults has led to the development of volume-targeted modes of ventilation for neonates.1–8 The pressure required to inflate the lungs of very preterm infants varies considerably owing to changes in their lung disease, the size of their spontaneous breaths, surfactant treatment, the use of uncuffed endotracheal tubes with a variable leak and different ventilation strategies. Volume guarantee (VG) ventilation aims at ensuring a consistent expiratory tidal volume by varying the peak inflating pressure (PIP) for each inflation.
VG is a time-cycled, pressure-limited, mode of ventilation on the Dräger Babylog 8000 plus (Dräger Medical, Lübeck, Germany). It measures each expired tidal volume (VTe) and alters the PIP for the next inflation to try to maintain the VTe at a level that has been set by the operator. When the VTe delivered is less than the set VTe the ventilator increases the PIP for the next inflation. If the VTe is larger than the set VTe the PIP is reduced for the next inflation. According to the manufacturer’s information each change in PIP does not exceed 3 cm H2O. To compensate for variability in the infant’s respiratory effort, lung compliance and leaks around the endotracheal tube, the ventilator continuously modulates the PIP to control the VTe. Therefore the VG mode delivers a mean VTe very close to the set VTe.3 ,7 ,9–12
At the Royal Women’s Hospital, Melbourne, neonates are ventilated with the Dräger Babylog 8000 ventilator using assist control and VG modes. Assist control is used because in this mode each of the infant’s inspirations can trigger an inflation. A large screen on each ventilator shows flow, volume and pressure waves. We observed occasional wide fluctuations in the PIP from one inflation to the next that sometimes exceeded the manufacturer’s limit of 3 cm H2O from one inflation to the next. While investigating these changes in PIP we were informed by the manufacturers that the VG program controls the PIP independently for triggered and untriggered inflations and if the change in PIP from one inflation to the next exceeded 3 cm H2O this was probably owing to a change from a triggered to an untriggered inflation.
For triggered inflations the PIP chosen by the ventilator for each inflation relates to the PIP used for the previous triggered inflation, even if that occurred many inflations before. Similarly, the PIP for untriggered inflations relates to the PIP for the previous untriggered inflation. There is no time limit on the ventilator’s memory for the PIP for the previous triggered or untriggered inflations. This independent control of PIP for the two types of inflation is important because when an infant inspires, contributes to the VTe and triggers an inflation, a lower PIP would be appropriate to assist the infant and deliver the set VTe. Conversely, during inflations where the infant is apnoeic and not contributing to the VTe, the inflation is not triggered and the VTe is dependent on the PIP. This means that triggered and untriggered inflations may have very different PIPs even if they are adjacent and might vary by more than 3 cm H2O.
This study aimed at investigating the effects of the infant’s spontaneous breathing efforts and triggered or untriggered inflations on PIP and VTe.
METHODS
These data were collected as part of an audit of neonatal ventilation at the Royal Women’s Hospital, Melbourne. The research and ethics committees agreed this could be done with verbal parental consent, as there was no interference with the infant or ventilator. A convenience sample of clinically stable infants was studied if the infant was not sedated or muscle relaxed, weighed >500 g, was <38 weeks’ gestation and was ventilated with the Dräger Babylog 8000 using VG, assist-control (synchronous intermittent positive pressure ventilation) mode. Infants were not studied if they had a major congenital abnormality, periventricular leucomalacia or seizures. They were also excluded if there was an endotracheal tube leak >60% of the inspiratory tidal volume because the VG mode becomes inaccurate above this level. Following local protocols infants were started with a set VTe of 5 ml/kg, inspiratory time of 0.3 seconds, rate ∼60/minute, maximum PIP 30 cm H2O, positive end expiratory pressure (PEEP) 5 cm H2O, circuit flow 8 l/min and maximum trigger sensitivity. Where possible the Paco2 was maintained between 5 and 8 kPa (38–60 mm Hg) by adjusting the set VTe. Flow and pressure waves were recorded from the ventilator analogue outputs at 200 Hz using the Spectra program (Grove Medical Ltd, London, UK). The flow wave was integrated to tidal volume.
Another study using these recordings has been reported.7 Basic demographic information and ventilator settings were recorded at the start of each study. Each study was timed to coincide with routine blood gas analysis that was used to establish adequacy of ventilation and calibrate the transcutaneous blood gas monitor. Infants were not handled during the 30-minute recording and no changes were made to ventilator settings during this time. Simultaneous video recording was used to identify 10-minute epochs for analysis when the infant was not crying or moving.
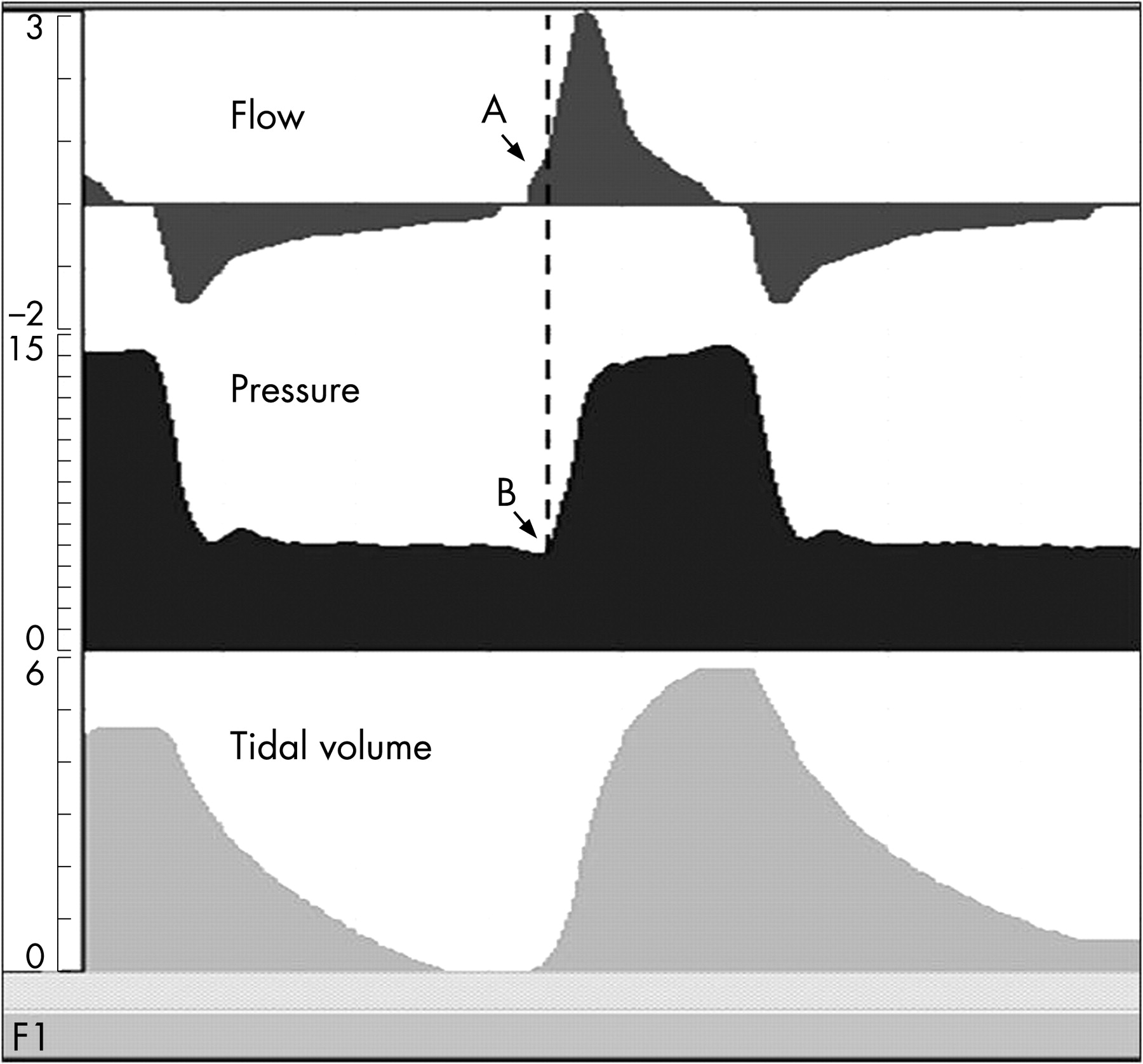
The flow, volume and pressure waveforms were examined and analysed for each inflation both manually and using a Labview 5.0 (National Instruments, Austin, USA) program, designed by one of the authors.13 To analyse triggered and untriggered inflations separately inflations were identified as triggered if: (a) inspiratory gas flow preceded the start of the increase in inflating pressure; (b) this coincided with a small dip in the pressure wave and (c) the interval between inflations was less than that set on the ventilator (fig 1).

Normally distributed data were compared using the Student t test and presented as mean and standard deviation. Non-parametric data were compared using Mann–Whitney U analysis and presented as median and range.
RESULTS
Ten infants ventilated through an endotracheal tube were studied for 30 minutes each, and 10 minutes of movement-free recording selected from each study. About 600 consecutive inflations were analysed in detail for each infant. In total 6540 inflations were analysed. Of these, 4052 (62%) were triggered and 2488 (38%) not triggered. Figure 2 illustrates the appearance of triggered and untriggered inflations.

{kind=link}
{kind=link}
The infants’ characteristics, median (range), were: gestational age 28 (24–37) weeks, weight 1275 g (630–3110 g), day of life when studied 3 (1–24), set VTe at the time of the study 3.85 (2.8–4.7) ml/kg and fractional inspired oxygen 0.28 (0.21–0.80). All had acceptable blood gases and maintained adequate ventilation and oxygenation throughout: mean (SD) SpO2 96 (3) %, TcCO2 6.2 (1.3) kPa (48 (10) mm Hg) and heart rate 142 (14) beats/min.
Effect of triggered and untriggered inflations on peak inflating pressure
Overall triggered inflations (n = 4053) had a lower PIP at 12.9 (4.9) cm H2O than untriggered inflations (n = 2488) at 17 (3.5) cm H2O (p<0.001). The mean (95% CI) PIP for triggered inflations was significantly lower than for untriggered inflations by 4.1 (3.9 to 4.3) cm H2O. When triggered inflations were immediately followed by an untriggered inflation (n = 838) the peak inflating pressure increased by a mean (SD) of 5.1 (6.7) cm H2O. When untriggered inflations (n = 839) were followed by a triggered inflation the PIP fell by 4.8 (6.7) cm H2O.
Between adjacent triggered inflations (n = 3209) the change in PIP was 0.11 (1.50) cm H2O and between adjacent untriggered inflations (n = 1644) it was 0.06 (1.53) cm H2O. Therefore pressure changes between inflations of the same type were less than 3.0 cm H2O for 97.7% of the time.
Effect of triggered and untriggered inflations on expired tidal volume
Despite the differences in PIP between the two types of inflations there was no significant difference between the delivered VTe as a percentage of the set VTe: triggered 103% and untriggered 101%.
When triggered inflations were immediately followed by an untriggered inflation (n = 838) and the PIP increased the VTe rose by 0.23 (2.06) ml/kg. When untriggered inflations were followed by a triggered inflation (n = 839) the VTe fell by 0.26 (2.19) ml/kg.
The change in VTe between adjacent triggered inflations (n = 3209) was 0.04 (1.22) ml/kg and between adjacent untriggered inflations (n = 1644) it was 0.09 (1.41) ml/kg.
The set maximum PIP of 30 cm H2O might have limited some of the inflating pressures. However, only 0.2% of the inflating pressures reached the set PIP.
DISCUSSION
We report a detailed analysis of changes in PIP and expired tidal volume for individual triggered and untriggered inflations during VG ventilation with the Dräger Babylog 8000 ventilator. This has not been possible in other studies of volume ventilation where the data have not been acquired in detail for individual inflations but have been averaged over varying periods.6 ,11 ,14
What is already known on this topic
Volume guarantee ventilation delivered by the Dräger Babylog 8000 plus ventilator is a pressure-limited, time-cycled, triggered mode that targets a set expired tidal volume by altering the peak inflating pressure for each inflation.
These pressure changes should not exceed 3 cm H2O between inflations according to the manufacturers.
The effect of triggered and untriggered inflations on the inflation pressures and tidal volumes has not been reported.
Volume-targeted modes of neonatal ventilation are used to reduce volutrauma and associated ventilator-induced lung injury that has been linked to the development of bronchopulmonary dysplasia.2 A meta-analysis comparing volume-targeted ventilation with traditional time-cycled, pressure-limited modes has shown reductions in the duration of ventilation, rates of pneumothorax and severe intraventricular haemorrhage, and shows a trend towards a reduction in the incidence of bronchopulmonary dysplasia (relative risk = 0.34 (95% CI 0.11 to 1.05)).15
What this study adds
Between inflations of the same type (triggered or untriggered) the change in peak pressure between consecutive inflations in less than 3 cm H2O.
When a triggered inflation is immediately adjacent to an untriggered inflation the change in peak pressure can be around 5 cm H2O.
Although triggered inflations have a peak pressure 4 cm H2O lower than untriggered inflations this makes no difference to the expired tidal volumes.
When triggered and untriggered inflations were analysed separately (ie, the pressure for a triggered inflation compared with an adjacent triggered inflation, and similarly for untriggered inflations), the differences were within the manufacturer’s 3 cm H2O limit for both types for 97% of the time. However, pressure fluctuations above 3 cm H2O occurred between consecutive inflations when the inflations changed between triggered and untriggered modes. Triggered inflations, where the infant contributed to the tidal volume, were delivered with a PIP about 4 cm H2O lower than untriggered inflations.
The difference in PIP between triggered and untriggered inflations is due to the presence or absence of infant inspiratory effort. During an untriggered inflation the infant is not inspiring and so the ventilator pressure has to be sufficient to provide the set tidal volume. During a triggered inflation the infant is inspiring and contributing to the tidal volume. The VG program adjusts the peak pressure to ensure a set expired tidal volume and so the pressure needed to ensure the tidal volume with a triggered inflation is lower than with an untriggered inflation. This change in peak pressure inflation does not occur with time-cycled, pressure-limited ventilation in assist-control mode.
Our own observations have shown that pressure-limited ventilator modes which do not control the tidal volume deliver a fixed PIP independent of the infant’s respiratory effort. This results in very large changes in tidal volume as the infant varies their spontaneous tidal volume or the lung compliance changes.
In this study only 62% of the inflations were triggered because the set ventilator rate of 60/min was close to the infant’s spontaneous respiratory rate; this reduced the infant’s ability to trigger the ventilator because a mandatory, or back-up inflation, was delivered before the infant had time to inspire. Our recent experience has been that with a ventilator rate lower than 60/min the proportion of triggered inflations increases. This is likely to improve the overall effect of VG ventilation when the baby is breathing spontaneously and triggering inflations.
The information in this study is specific to the Dräger Babylog 8000 plus ventilator. Other neonatal ventilators, with other methods of controlling tidal volume do not have the same control algorithms for triggered and untriggered modes, nor do they all target the expiratory tidal volume.
CONCLUSION
During VG ventilation with the Dräger Babylog 8000 the PIP was 4 cm H2O lower during triggered inflations than untriggered inflations, although the expired tidal volumes were similar. The fluctuations in inflating pressures during VG ventilation are an integral part of providing consistent expiratory tidal volumes for ventilated infants with variable inspiratory effort.
Acknowledgments
Peter Dargaville and Naomi McCallion were holders of a Murdoch Children’s Research Institute Senior Research Fellowship and a Royal Women’s Hospital Research Fellowship, respectively.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Fantoms