Article Text

Abstract
Objetive To determine whether full-term newborn infants of diabetic mothers (IDM) present immature/disorganised EEG patterns in the immediate neonatal period, and whether there was any relationship with maternal glycaemic control.
Design and setting Cohort study with an incidental sample performed in a tertiary hospital neonatal unit.
Patients 23 IDM and 22 healthy newborns born between 2010 and 2013.
Interventions All underwent video-EEG recording lasting >90 min at 48–72 h of life.
Main outcome measures We analysed the percentage of indeterminate sleep, transient sharp waves per hour and mature-for-gestational age EEG patterns (discontinuity, maximum duration of interburst interval (IBI), asynchrony, asymmetry, δ brushes, encoches frontales and α/θ rolandic activity). The group of IDM was divided into two subgroups according to maternal HbA1c: (1) HbA1c≥6% and (2) HbA1c<6%.
Results Compared with healthy newborns, IDM presented significantly higher percentage of indeterminate sleep (57% vs 25%; p<0.001), discontinuity (2.5% vs 0%; p=0.044) and δ brushes in the bursts (6% vs 3%; p=0.024); higher duration of IBI (0.3 s vs 0 s; p=0.017); fewer encoches frontales (7/h vs 35/h; p<0.001), reduced θ/α rolandic activity (3/h vs 9/h; p<0.001); and more transient sharp waves (25/h vs 5/h; p<0.001). IDM with maternal HbA1c≥6% showed greater percentage of δ brushes in the burst (14% vs 4%; p=0.007).
Conclusions Full-term IDM newborns showed video-EEG features of abnormal development of brain function. Maternal HbA1c levels<6% during pregnancy could minimise the risk of cerebral dysmaturity.
- Clin Neurophysiology
- Diabetes
- Neonatology
- Neurodevelopment
- Fetal Medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
What is already known in this topic
-
Infants of diabetic mothers (IDM) present lower IQ scores, motor and language disorders, attention deficit and hyperactivity later in life.
-
Visual, auditory and somatosensory evoked potentials, and event-related potentials carried out in IDM showed significantly delayed mean latency in all of them.
-
There are no standard video-EEG studies on full-term newborn IDM that assess brain functional development in the immediate neonatal period.
What this study adds
-
Even with good glycaemic control during pregnancy, infants of diabetic mothers (IDM) present video-EEG findings of delayed development of brain function from birth.
-
Full-term newborn IDM also show excessive transient sharp waves suggesting a subacute/chronic brain lesion.
-
Maternal HbA1c levels <6% during pregnancy could minimise the risk of cerebral immaturity at birth in these infants.
Introduction
Although most infants of diabetic mothers (IDM) are asymptomatic at birth, they present lower capacity for habituation to auditory stimuli in foetal and neonatal life,1 lower IQ scores and impaired verbal development later in life, as well as a higher incidence of motor and language disorders, attention deficit and hyperactivity.2–4 All these effects are negatively correlated with maternal glycaemic control.5 However, ‘good maternal metabolic control’, the result of close monitoring of maternal blood glucose levels with glycosylated haemoglobin (HbA1c) <5% until just before delivery, is insufficient to ensure normal oxygenation and metabolic status of the foetus in mothers with gestational diabetes.6
Neuropsychological assessment carried out in IDM to date includes visual, auditory and somatosensory evoked potentials, and event-related potentials. IDM showed significantly delayed mean latency in all of them.7 Moreover, IDM present other developmental anomalies such as inattention, hyperactivity and fine and gross motor deficits which may be common to other insults such as hypoxia-ischemia or prematurity.
We have found only one old study on IDM neonates involving standard EEG8 ,9; the authors found immature EEG patterns and behaviour in some IDM during sleep. Immature EEG patterns are sometimes observed in non-IDM neonates, without a clear aetiology. In some cases, such patterns may be due to other adverse intrauterine conditions such as undernutrition10 which may constitute a slight but persistent brain insult. Preterm infants with persistent immature EEG patterns at term conceptional age (CA) showed significantly lower global and verbal IQ than those without such patterns.11
Our objective was to assess, in the immediate neonatal period, the influence of possible insult due to diabetes during pregnancy on infant brain development by using visual EEG analysis, and whether there was any relationship with maternal glycaemic control. We hypothesised that full-term newborn IDM would present more features of EEG dysmaturity than CA-matched infants of non-diabetic mothers in the immediate neonatal period.
Patients and methods
Design
Cohort study.
Patients
The diabetic mothers participating in this study were recruited from our hospital Fetal Pathophysiology Unit, which monitored each pregnancy. The unexposed cases were selected in the delivery ward of the same hospital. Between January 2010 and January 2013, we recruited 23 newborns of mothers with pregestational type 1 diabetes and a control group of 22 healthy newborns. HbA1c was determined in all diabetic mothers at least at the first visit (first trimester) and halfway through the second and third trimesters of pregnancy. The inclusion criteria for both groups were gestational age (GA) >37 weeks, single pregnancy, cephalic presentation, ultrasound-estimated foetal weight >10th percentile and normal amniotic fluid test, no resuscitation in the delivery room, Apgar score >7 at 5 min, and normal umbilical cord pH (>7.1). The exclusion criteria for both groups were maternal body mass index (BMI) <20 or >30 at the start of pregnancy, chronic pathology other than maternal diabetes (epilepsy, moderate/severe asthma etc.), obstetric pathology (hypertension, metrorrhagia, etc), maternal toxic habits (smoking, alcohol, drugs), birthweight <2.5 kg, congenital malformations or chromosomal abnormalities, and admission to the neonatal unit for special care (ie, phototherapy, glucose supplements, ventilatory and/or oxygen support, etc).
Informed consent was obtained from the mothers. All newborn infants underwent Amiel-Tison neurological assessment12 at 2–3 days of postnatal life. Only those with normal results were included in this study. GA was calculated according to last menstrual period and confirmed by prenatal ultrasound at first trimester.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Ethics Committee of our hospital.
Methods
EEG recording
All newborns underwent video-EEG recording at 48–72 h of life, during >90 min to record at least one complete sleep–wake cycle. We used a portable digital video-EEG (XLTEK 2568 by Bristol Circle), incorporating XLDB Software V.6.0.0 Build 632 for video-EEG recording. Several montages were used with electrodes placed according to the international 10/20 system adapted for neonates. The recording also included five polygraph channels: two for eye movements, one for chin muscle activity, one for chest movement and one for the electrocardiogram.
Electrode impedance was maintained at <10 Ω. We used helmets of different sizes by applying conductive gel electrodes (Electro-gel; OJ Electro-cap International). Any EEG activity that could not be defined as a normal or abnormal pattern was identified as gross artefact and excluded from the analysis.
All video-EEG recordings were evaluated separately by two experienced neonatologists (DGB and CGC), who were blinded as to the study groups (healthy controls vs IDM). We accepted an EEG feature only when the two evaluators were in agreement.
Visual analysis and data collection
Sleep state differentiation
The states of active, quiet and indeterminate sleep were established by observed concordance between body motility, eye movements and cardio-respiratory patterns throughout video-polygraphic recording. The three sleep states were defined following previous recommendations.13 ,14 Indeterminate sleep was defined as any state not classified as active or quiet sleep, with the same behaviour and EEG pattern maintained during ≥3 min.
EEG visual analysis
Mature-for-GA parameters
Discontinuous pattern, interburst interval (IBI) of inactivity or hypoactivity, asynchrony, asymmetry and δ brushes were measured as described in a previous study by our team15 (figure 1A). We considered discontinuous pattern as IBI in all EEG channels showing amplitude <30 µV during >1 s (normal in preterm infants with GA <36 weeks) and tracé alternant as IBI amplitude >30 µV in all EEG channels (normal in full-term newborn infants).
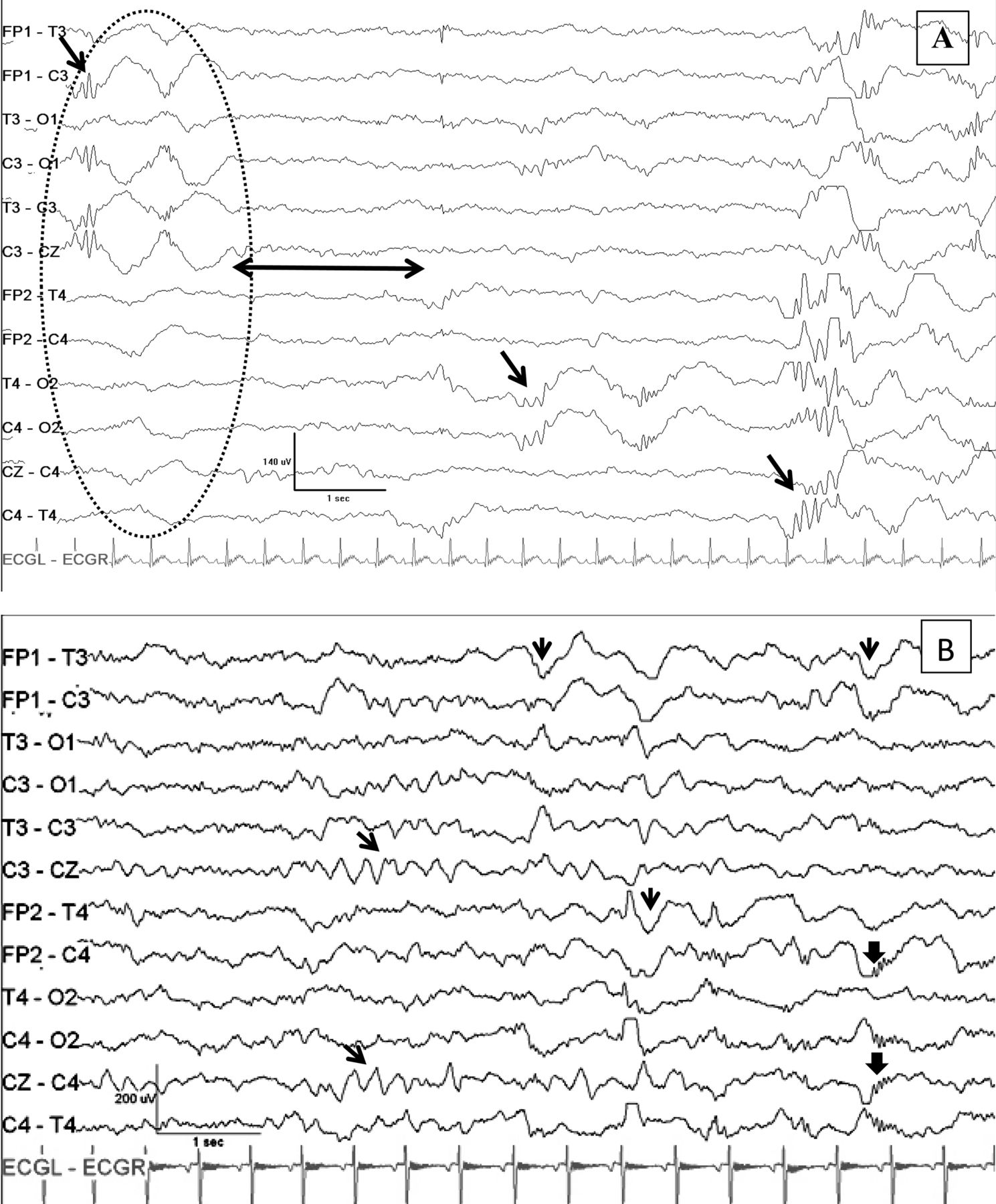
(A) Discontinuous EEG tracing during quiet sleep in an infants of diabetic mothers (IDM) showing hypoactivity (arrow with two heads), asymmetry (inside the oval, the top six channels correspond to the left hemisphere and the bottom six channels correspond to the right hemisphere), and with δ brushes in the two bursts with characteristic rapid activity superimposed on the ascending slope of a δ wave (arrow). (B) Continuous pattern in a healthy neonate during quiet sleep with a burst of α/θ rolandic activity (inclined arrows), encoches frontales (vertical arrows) and large slow waves with superimposed rapid activity (wide vertical arrows).
EEG patterns specific to term GA
Encoches frontales: Biphasic frontal sharp waves with initial negative deflection followed by a positive deflection where the wave is wider and of greater amplitude (figure 1B). Amplitude varies between 50 and 200 µV and duration from 0.5 s to 0.75 s. We recorded the total number of encoches frontales per hour when synchronous on frontal areas of both hemispheres.
α/θ rolandic activity (A/TRA): Bursts of α or θ waves of short duration (<5 s) located in rolandic areas. We recorded the total number per hour of sleep.
Transient sharp waves (TSW)
These were defined as in previous publications,16–18 according to location. We counted the total number of TSW per hour.
Statistical analysis
The results of this cohort study, with an incidental sample of 45 newborn infants, are expressed as means and SD. Comparisons between pairs of groups for continuous variables were performed using Mann–Whitney U test. Correlations between continuous variables were performed using Spearman's r test (two-sided). We did not identify any confounders. We addressed the problem of multiple comparisons with Bonferroni correction (α/k, where α is 0.05 and k is the number of tests).
IDM were categorised using a cut-off value ≥6% HbA1c. To compare EEG variables between the two subgroups (higher vs lower than 6%), we used Mann–Whitney U test. Differences with a p value <0.05 were considered statistically significant. All statistical analysis was performed using SPSS V.17.0 (Chicago, Illinois, USA).
Results
Perinatal data of both groups are shown in table 1. All diabetic mothers had HbA1c levels <7%, except four. Two of these women reduced their levels to <7% in the second and third trimesters. Although weight gain in pregnancy was similar in both groups, 17 diabetic mothers had high BMI (>25) at the start of pregnancy compared with only six non-diabetic mothers.
Perinatal data and birthweight of neonates
Figure 2A shows comparative results of EEG discontinuity, IBI, asymmetry and asynchrony between the two groups. The percentage of discontinuity of the total sleep EEG recording was 0.6% (range 0–11) in controls versus 2.5% (range 0–32) in IDM (p=0.044) (Five controls had discontinuous EEG tracing at some time, compared to 13 IDM); maximum duration of IBI in seconds was 0.0 (range 0–1.8) in controls versus 0.3 (range 0–5.9) in IDM (p=0.017); the percentage of asynchrony of total sleep EEG recording was 4.0% (range 0–14) in controls versus 5.7% (range 0–18) in IDM (p=0.068); and the percentage of asymmetry was 2.8% (range 0–11) in controls versus 4.8% (range 0–17) in IDM (p=0.467).

Boxplot showing comparative results of all EEG variables between controls and infants of diabetic mothers (IDM): (A) percentage of discontinuity, maximum duration of interburst interval (IBI) and percentage of bursts with asymmetry and asynchrony; (B) percentage of indeterminate sleep of total sleep, number of transient sharp waves (TSW) per hour and percentage of bursts with δ brushes; (C) percentage of quiet sleep with tracé alternant, number of encoches frontales and bursts of α/θ rolandic activity (A/TRA) per hour. *=NS; †=p<0.05; ‡=p<0.01.
Figure 2B shows comparative results of the percentage of indeterminate sleep, number of TSW per hour and percentage of bursts with δ brushes between controls and IDM. The percentage of indeterminate sleep was 25% (range 0–72) in controls versus 57% (range 20–78) in IDM (p<0.001); the percentage of δ brushes in the bursts was 3% (range 0–25) in controls versus 6% (range 0–54) in IDM (p=0.024), and δ brushes were absent in four IDM and in six controls; the number of TSW per hour was 5 (range 0–8) in controls versus 25 (range 1–49) in IDM (p<0.001). The number of TSW per hour in the temporal area was 3 (range 0–13) in controls versus 16 in IDM (range 3–46) (p<0.001); in the rolandic area, 2 (range 0–6) in controls versus 7 (range 0–21) (p<0.001); in frontal and occipital areas, <3 (range 0–10) in both groups without significant differences.
Figure 2C shows comparative results of the percentage of quiet sleep with tracé alternant, number of encoches frontales and bursts A/TRA per hour between the two groups. The percentage of tracé alternant during quiet sleep was 37 (range 0–79) in controls versus 20 (range 0–53) (p<0.001). Only one IDM showed no tracé alternant. The duration of tracé alternant was over 50% of total sleep time in only one IDM compared with six of the controls; the number of encoches frontales per hour was 35 (range 5–87) in controls versus 7 (range 7–40) in IDM (p<0.001). All the newborns presented encoches frontales, except one IDM; the number of A/TRA per hour was 9 (range 0–76) in controls versus 3 (range 0–21) in IDM (p<0.001). A/TRA was recorded in 15 IDM and in 21 of the 22 controls.
Spearman's correlations between TSW per hour and other EEG variables were determined. We found significant positive correlation with percentage of indeterminate sleep (r 0.388, p=0.019). Significant negative correlations were found with tracé alternant (r −0.491, p<0.001), encoches frontales (r −0.466, p<0.001) and A/TRA (r −0.436, p<0.004).
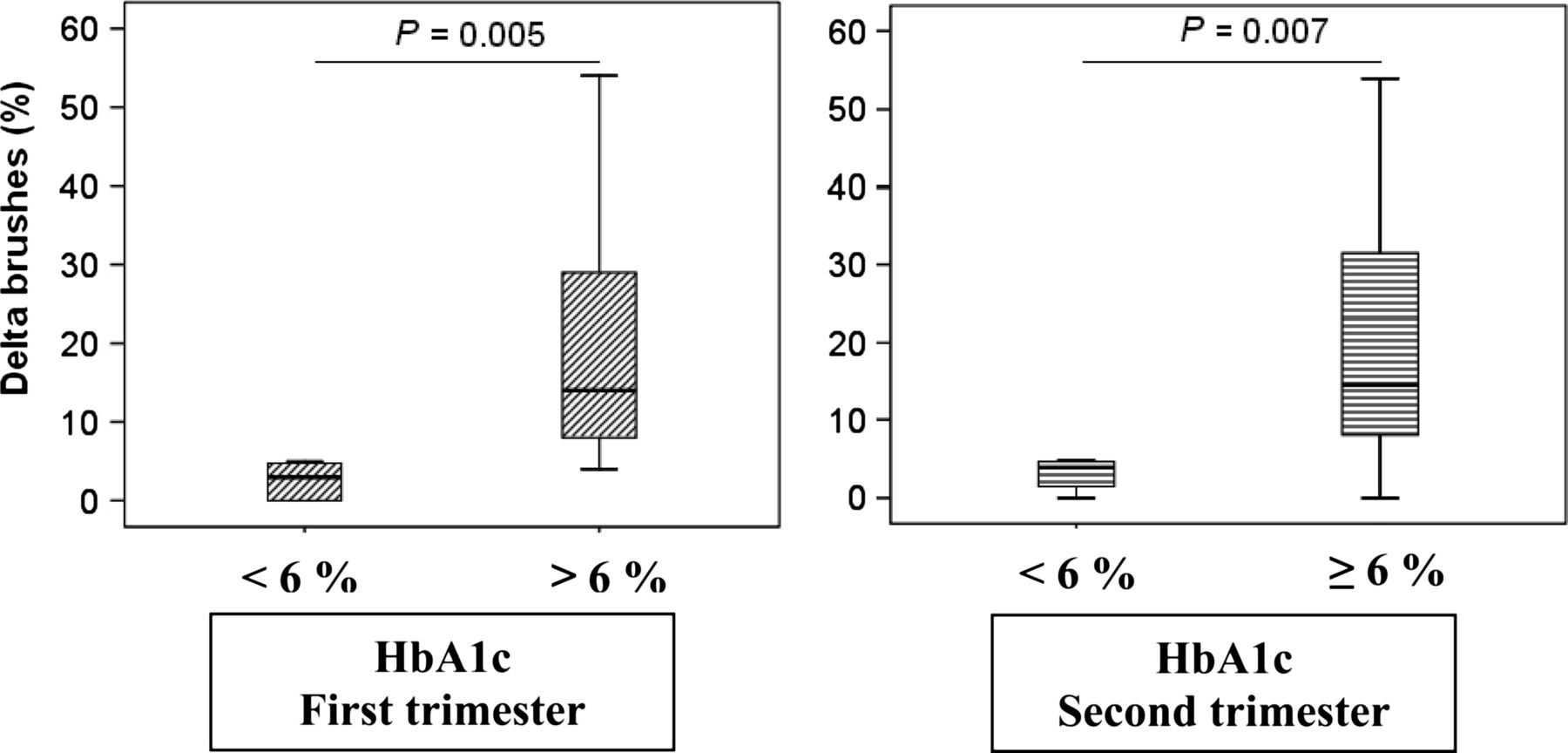
On considering only IDM, maternal BMI had no significant correlation with any of the EEG data analysed. However, HbA1c showed a significant positive correlation with a higher percentage of δ brushes in the bursts (p=0.004, p<0.001 and p=0.046 in the first, second and third trimester, respectively). Using a cut-off of ≥6% HbA1c (12 diabetic mothers in the first, ten in the second and nine in third trimester, respectively), we found a higher percentage of δ brushes in the group with maternal HbA1c≥6% in the first and second trimester of pregnancy (14% vs 4% in both cases), which was highly significant (p=0.005 and p=0.007, respectively) (figure 3), but not in the third trimester.

{kind=link}
{kind=link}
{kind=link}
Comparison of the proportion of δ brushes in the burst in the EEG of infants of diabetic mothers (IDM) according to glycosylated haemoglobin (HbA1c) levels above or below 6% in the first and second trimester of pregnancy.
Discussion
Although in the present study, the apparently healthy term IDM had ‘good gestational control’ (HbA1c <7%),19 they showed a higher percentage of immature EEG patterns, a higher number of TSW, a higher percentage of indeterminate sleep and fewer EEG patterns considered normal at term GA (encoches frontales and A/TRA) compared with healthy term neonates. These EEG findings (dysmature or disorganised EEG patterns) have been described in preterm at term CA and term newborn infants with other pathological or non-pathological conditions. The EEG abnormalities of excessive TSW and dysmature EEG patterns have been associated with mild brain injury and cognitive deficits in later life.20
Dysmature EEG patterns have been described in preterm infants at term CA with chronic lung disease,21 in asymptomatic newborns with prenatal drug exposure22 and in premature newborns with extreme malnutrition and low weight10 without any other apparent cause of acute or chronic brain damage. All were associated with adverse neurological outcome.
Schulte et al8 ,9 studied 14 IDM neonates with GA between 36 and 41 weeks. They found significantly more immature and fewer mature EEG sleep patterns in IDM. They observed that the tracé alternant in quiet sleep contained many spikes with marked attenuation of activity between the bursts and many large slow waves with rapid activity superimposed, mimicking immature patterns. However, they only performed global EEG visual analysis to estimate GA and did not define either mature-for-GA parameters or specific EEG patterns.
We analysed EEG patterns considered normal for term GA, such as encoches frontales and A/TRA. The number of both these EEG patterns was significantly higher in healthy infants than in IDM. Encoches frontales appear at 35–36 weeks GA, decrease in frequency from week 3–5 of term age and are absent after week 8 of life in term neonates.23 A/TRA has been little studied since the work by Monod et al24. Later Hayakawa et al25 found bursts of Fz θ/α activity in 50% of healthy term infants versus only 4% of term infants with unfavourable developmental outcome. We therefore suggest that the decreases in these two EEG elements are signs of delayed cerebrocortical electrophysiological maturation in IDM.
We found a higher number of sharp waves in IDM compared to healthy neonates. Frontal, occipital and rolandic sharp waves have been reported as a sign of acute or subacute ischaemic lesion in premature newborns, with high sensitivity and specificity at 4–30 days of life after severe acute and extensive white brain matter lesion. From 1 month after the acute injury, these elements diminish and disappear.18 ,26 Positive temporal sharp waves also increase significantly with severe brain injuries, being prominent in week 2 of life and descending by week 4, but may occur in significant numbers (>10/h) at term age in premature infants of 31–32 weeks of gestation with severe brain injury.16 In the present study, full-term newborn IDM showed excessive temporal and rolandic TSW (>5/h). Therefore, our findings suggest persistent brain lesion rather than an acute or subacute lesion.
This increased number of TSW in our IDM was positively correlated with immature EEG patterns and negatively correlated with EEG patterns typical of normal full-term newborn infants. In preterm infants, excessive numbers of TSW have been associated with other dysmature or disorganised EEG patterns, implying poor prognosis.16 ,17 ,26 The same could be said about many of our term IDM; they may therefore also suffer developmental disorders described in preschool and school age children born to mothers with diabetes during pregnancy.
The cut-off value of 6% for HbA1c was chosen because this is considered the upper limit of normal range.19 HbA1c showed a highly significant positive correlation with a higher percentage of δ brushes in the bursts. In addition, when HbA1c was <6% in the first and second trimester of pregnancy, the percentage of δ brushes in the burst was significantly lower than those IDM whose mothers had levels of HbA1c ≥ 6%. As mentioned, HbA1c control is not sufficient to ensure normal oxygenation and metabolic status,5 but the present study suggests that HbA1c levels should be kept <6%, at least until better methods to monitor maternal metabolic status become available.
The limitations of the present study include (1) the small sample size, despite which significant results were obtained; (2) first trimester BMI was higher in diabetic mothers; however, in contrast to HbA1c, BMI bore no significant relationship with any EEG parameter and therefore had no influence on the results; and (3) higher birthweight in IDM than healthy neonates, but not a cause of labour complications in any case.
In conclusion, term IDM showed EEG patterns of maturational delay, had a higher percentage of indeterminate sleep in total sleep, and an increased number of TSW compared to healthy newborn infants without diabetic mothers. These video-EEG features could be signs of abnormal development of brain function (immaturity and/or brain lesion), which were reduced when HbAc1 levels were maintained <6%. We believe that these findings can only be the result of adverse intrauterine environment attributable to maternal diabetes during pregnancy.
Acknowledgments
Dr Alejandro Jiménez helped with statistical analyses and Michael McLean with the English version of the manuscript.
References
Footnotes
-
Contributors JRCC and NLGG conceived the study. JRCC, NLGG, DGB, CGC, YZH and ESC developed the study design. DGB, CGC, YZH and ESC were responsible for data acquisition. JRCC undertook the data analysis and drafted the paper. All authors contributed to revision of the manuscript. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. JRCC is guarantor for the study.
-
Competing interests None.
-
Ethics approval Clinical Ethics Committee of University Hospital of Canary Islands.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Video-EEG recordings are stored in the hard disk of the device used in this study, with a copy on an external memory, both available to the authors listed on the title page. Clinical and demographic data of the participating mothers and infants are stored in their respective medical records, and those data used in the present study are stored as Excel sheets. These data are only available to the authors listed.