Article Text

Abstract
Objective To evaluate the clinical course, respiratory outcomes and markers of inflammation in preterm infants with moderate respiratory distress syndrome (RDS) assigned from birth to nasal continuous positive airway pressure (NCPAP) or bi-level NCPAP.
Methods A total of 40 infants with a gestational age (GA) of 28–34 weeks (<35 weeks' GA), affected by moderate RDS, were considered eligible and were randomised to NCPAP (group A; n=20, CPAP level=6 cm H2O) or to bi-level NCPAP (group B; n=20, lower CPAP level=4.5 cm H2O, higher CPAP level=8 cm H2O), provided with variable flow devices. Inflammatory response was the primary outcome; serum cytokines were measured on days 1 and 7 of life. Length of ventilation, oxygen dependency, need for intubation and occurrence of air leaks were considered as secondary outcomes.
Results Infants showed similar characteristics at birth (group A vs group B: GA 30.3±2 vs 30.2±2 weeks, birth weight 1429±545 vs 1411±560 g) and showed similar serum cytokine levels at all times. Group A underwent longer respiratory support (6.2±2 days vs 3.8±1 days, p=0.025), longer O2 dependency (13.8±8 days vs 6.5±4 days, p=0.027) and was discharged later (GA at discharge 36.7±2.5 weeks vs 35.6±1.2 weeks, p=0.02). All infants survived. No bronchopulmonary dysplasia (BPD) or neurological disorders occurred.
Conclusions Bi-level NCPAP was associated with better respiratory outcomes versus NCPAP, and allowed earlier discharge, inducing the same changes in the cytokine levels. It was found to be well tolerated and safe in the study population.
Statistics from Altmetric.com
Introduction
Despite antenatal steroid treatment, mechanical ventilation and surfactant replacement therapy, bronchopulmonary dysplasia (BPD) still remains a major cause of mortality and morbidity in very preterm infants. Ventilator induced lung injury prevention may begin from birth, and respiratory support without endotracheal intubation is an attractive option.
Nasal continuous positive airway pressure (NCPAP) reduces the risk of reintubation and, when used in the acute phase of respiratory distress syndrome (RDS) in infants born at 25–28 weeks' gestational age (GA), it has been shown to reduce the length of oxygen dependency and length of ventilation (although it does not reduce the rate of death or BPD); the use of high levels of positive end-expiratory pressure (PEEP) was associated with a higher incidence of pneumothorax.1,–,3
What is already known on this topic
Some non-invasive respiratory supports reduce the rate of reintubation for very premature infants.
These supports may be used as the primary approach to acute moderate respiratory distress syndrome (RDS).
Proinflammatory cytokine alterations have been implicated in the pathogenesis of bronchopulmonary disease.
What this study adds
Bi-level nasal continuous positive airway pressure (NCPAP) induces the same changes in cytokine levels as conventional NCPAP.
There was a significantly longer need for respiratory support and O2 dependency in the NCPAP group.
Moreover, the early use of CPAP has been shown to be of advantage in reducing the need for mechanical ventilation (RR 0.55; 95% CI 0.32 to 0.96).4 However, several papers were not able to demonstrate the reduction of the need of mechanical ventilation associated with the use of NCPAP.
Efforts to reduce the NCPAP failure rate (mostly due to ongoing lung disease, apnoea of prematurity or progressive atelectasis) prompted the use of nasal intermittent positive pressure ventilation (NIPPV), which is well established in many paediatric conditions; the terminology surrounding NIPPV and other forms of non-invasive ventilations is confusing, since in the literature many terms, whose origin may be clinical, technical or linked to the different devices, are used to describe the same non-invasive support. Hence many terms used do not fit the definition.
Bi-level NCPAP is a non-invasive respiratory support, which is much more similar to CPAP than to ventilation; it provides two alternating levels of CPAP in order to switch the functional residual capacity (FRC) of the neonate between two different levels. The theoretical benefits of bi-level NCPAP are that FRC switching may recruit unstable alveoli (or prevent their collapse) with the generation of a tidal volume (Vt) by the δ pressure between two levels of CPAP, and offload some of the respiratory work. ‘Bi-level NCPAP’ is a term that, in our opinion, fits the definition well because it provides a phasic increase in pressure.
Mechanical ventilation plays a critical role in the physiopathology of ventilation induced lung injury (VILI), while barovolutrauma and oxygen toxicity trigger inflammatory responses (as shown by cytokine expression), an important mechanism leading to BPD in the immature lung.5
Proinflammatory cytokine alterations have been implicated in the pathogenesis of nearly every significant premature neonatal disease process, most notably in the modulation of brain, lung and gut injury. Recent data demonstrated the importance of increased levels of serum proinflammatory cytokines in sepsis and in moderate/severe forms of new BPD development.6,–,17
Migliori et al demonstrated that nasal bi-level positive airway pressure (BiPAP), as compared to NCPAP, improved gas exchange in the same cohort of preterm infants with repeated cycles of the two supports.18
As far as we know there have been no published reports comparing NCPAP and bi-level NCPAP with variable flow system in the treatment of the acute phase of moderate RDS, in terms of safety (inflammatory response) and efficacy (short-term clinical efficacy).
We hypothesised that early application of bi-level NCPAP in preterm infants with RDS may induce a different inflammatory response when compared with NCPAP, and may have a different effect on length of ventilation, oxygen dependency, need for intubation and occurrence of air leaks (secondary variables).
Methods
This study was performed in a tertiary level neonatal intensive care unit (NICU) in 2007–2008 in Milan, Italy. Infants of 28–34 weeks' gestational age, inborn, affected by moderate RDS, were considered eligible. Infants with lethal congenital anomalies or requiring muscle relaxant, severe intraventricular haemorrhages (intraventricular haemorrhage (IVH) > grade II), chorioamnionitis, sepsis (positive blood culture) or suspected infection (eg, prolonged rupture of membranes, mother fever) were excluded. Written informed parental consent was obtained in the delivery room, during the prenatal interview, or in the first hour of life (table 1).
Consort fl ow diagram of the trial
Moderate RDS was diagnosed within the first hour of life on radiological and clinical criteria (a/APO2 ratio range for the definition of moderate RDS was 0.3–0.35; before randomisation, within the first hour of life; each patient underwent chest x-ray).
After delivery all neonates underwent the same management, following our NICU protocol: initial stabilisation was provided in the delivery room by sustained inflations using a pressure level of 20–25 cm H2O for 10–15 s (by a flow controlled, pressure limited mechanical device specifically designed for neonatal resuscitation (Neopuff; Fisher & Paykel Healthcare, Auckland, New Zealand)). This was then reduced to a pressure level of 5 cm H2O and with the minimal fractional inspired oxygen concentration (FiO2), to maintain an oxygen saturation (SpO2) of 85% up to 93% (or up to 95% in larger infants).19 Subsequent FiO2 adjustment and weaning and (SpO2) monitoring followed our NICU protocols.
Endotracheal porcine natural surfactant (Curosurf, 200 mg/kg); Serono, Geneva Switzerland was administered with the INSURE (for ‘INtubation–SURfactant administration–Extubation’) method if the preset criteria of the NICU protocols were met.
All infants enrolled in the study were sequentially numbered after birth and were randomised at 1 h of life to the NCPAP group (group A) or bi-level NCPAP group (group B) (Infant Flow CPAP vs Infant Flow synchronized inspiratory positive airway pressure (SiPAP); Viasys Healthcare, Yorba Linda, California, USA) using a table of random numbers and using a stratified randomisation for gestational age (GA 28–31 weeks; GA 32–34 weeks).
The four parameters to be adjusted during the use of the bi-level NCPAP were as follows: (1) lower CPAP level (indicated on the SiPAP device as ‘Pres low’); (2) upper CPAP level (indicated on the SiPAP device as ‘Pres high’); (3) time high (Thigh), the time of maintenance of upper CPAP level (indicated on the SiPAP device as ‘Ti’); (4) pressure exchange rate, (indicated on the SiPAP device as ‘Rate’). The Infant Flow SiPAP device provides variable flow bi-level NCPAP.
Short binasal prongs were used in both groups and the prong size used was the largest one that would fit the infant's nares without blanching the surrounding tissue. In group A, we set a CPAP level of 6 cm H2O. Weaning occurred following NICU protocols with the progressive reduction of the set CPAP level. In group B we set a lower CPAP level of 4.5 cm H2O and an upper CPAP level of 8 cm H2O, with Thigh set at 0.5–0.7 s with a pressure exchange rate of 30 times/min to start. Weaning occurred following NICU protocols with progressive reduction of the set pressure exchange rate (minimum 15 pressure exchanges/min) and, subsequently, with the reduction of the upper CPAP level (minimum upper CPAP level 6 cm H2O).
In both groups, during respiratory support or in spontaneous breathing, we set a minimal fractional inspired oxygen concentration (FiO2) to maintain oxygen saturation in the suggested limits.19
Intubation criteria were arterial pH<7.20, PaO2 <50 mm Hg with FiO2 >0.50 and PaCO2 >65 mm Hg, or >4 episodes of apnoea in 1 h or >2 episodes of apnoea in 1 h requiring repeated stimulation or bag-and-mask ventilation despite adequate prong fixing and CPAP delivery. Mechanical ventilation was stopped when FiO2 was <0.40, mean airway pressure (MAP) was <6 cm H2O, and PaO2 and PaCO2 were >50 and <65 mm Hg, respectively. The extubation of mechanically ventilated infants was mandatory within 2 h after they reached extubation criteria.
Similar blood gas goals were achieved to wean babies from respiratory support in both groups, as per our NICU protocols. CPAP was discontinued when neonates with adequate spontaneous respiratory effort had FiO2 <0.30, PEEP ≤4 cm H2O, PaO2 >50 mm Hg and PaCO2 <65 mm Hg.
Heart rate, systemic blood pressure and oxygen saturation were continuously monitored while arterial blood gas tension measurements (Radiometer Copenhagen, model ABL 700) were performed from an indwelling catheter or by capillary puncture.
The following data were also recorded: length of ventilation meant as total duration of respiratory support, incidence of patency of ductus arteriosus (PDA) and rate of medical treatment with ibuprofen, surfactant treatment (number of doses needed), incidence of air leaks (number of cases of pneumothorax), occurrence of IVH ≥1, oxygen dependency on day 28 and/or at 36 weeks' post-conceptional age and survival.
Cerebral ultrasound (US) was performed in the first 3 h of life. Subsequent x-rays were performed as needed, while cerebral US was performed on days 1, 3, 7, 15, 28 and at 36 weeks of GA. Within 24 h of life an echocardiographic evaluation was performed in order to ascertain PDA status, which if positive was treated with ibuprofen: 10 mg/kg extravenously, followed by another two doses of 5 mg/kg intravenously at 24 h intervals.
Cytokines planned for measurement included interleukin (IL)6 (early peak), as it is an early marker of inflammation, IL8, as it is the most important chemotactic factor in the lung, and tumour necrosis factor (TNF)α (later peak) as it seems to play a role in maintaining chronic inflammation in BPD, utilising a solid-phase, two-site chemiluminescent immunometric assay with automated analyser (Immulite; Medical Systems, Genova, Italy).15 Blood samples were collected in stable newborns on day 1 (day of birth, after surfactant administration but prior to randomisation) and day 7. All the samples (1 ml) were centrifuged (for 5 min at 3000/rpm) before assay in order to obtain 500 µl of serum.
All samples expected to have cytokines concentration higher than calibration range (up to 1000 pg/ml for TNFα and for IL6; up to 7500 pg/ml for IL8) were diluted with a specific sample diluent before assay to reduce the possible difference in collection volumes.
For each measurement, 50–150 µl of serum were used, with a sensitivity of 5 pg/ml for IL6, 2 pg/ml for IL8 and 1.7 pg/ml for TNFα. When immediate measurement of cytokines was impossible, samples were stored at 2–8°C for up 2 days, at −20°C for longer periods of time.
The research protocols were approved by the V.Buzzi Children's Hospital Ethics Committee.
Data acquisition and analysis
We calculated a sample size of at least 15 neonates was required in each group to find a difference of 50% in serum IL6, IL8 and TNF in the two groups at 7 days of life, with 80% power at the 0.05 level. Normally distributed data were compared with use of the unpaired Student t test and non-parametric outcomes with use of the χ2 test. Data within each group were compared by analysis of variance (ANOVA; Bonferroni post hoc). Statistical significance was at the p<0.05 level. Staff in the NICU were not blinded to the treatment. All cytokine samples were analysed in duplicate by laboratory staff unaware of the ventilatory strategies, and the results were communicated to the investigators at the end of the analysis.
Results
In all, 44 infants were considered eligible; 4 were excluded for chorioamnionitis, suspected sepsis or lack of parental consent. A final total of 40 infants were studied and randomised at 1 h of life to group A (NCPAP) (n=20) and to group B (bi-level NCPAP) (n=20) (table 1).
Table 2 shows the clinical characteristics of the infants; we did not observe significant differences between the two groups. The respiratory and ventilatory status of each group at the time of the randomisation was similar. No steroids were given in the first week of life. FiO2 administered at the time of the randomisation did not differ between the two groups.
Characteristics of infants in group A (nasal continuous positive airway pressure (NCPAP)) and group B (bi-level NCPAP) at the time of randomisation (values expressed as mean±SD)
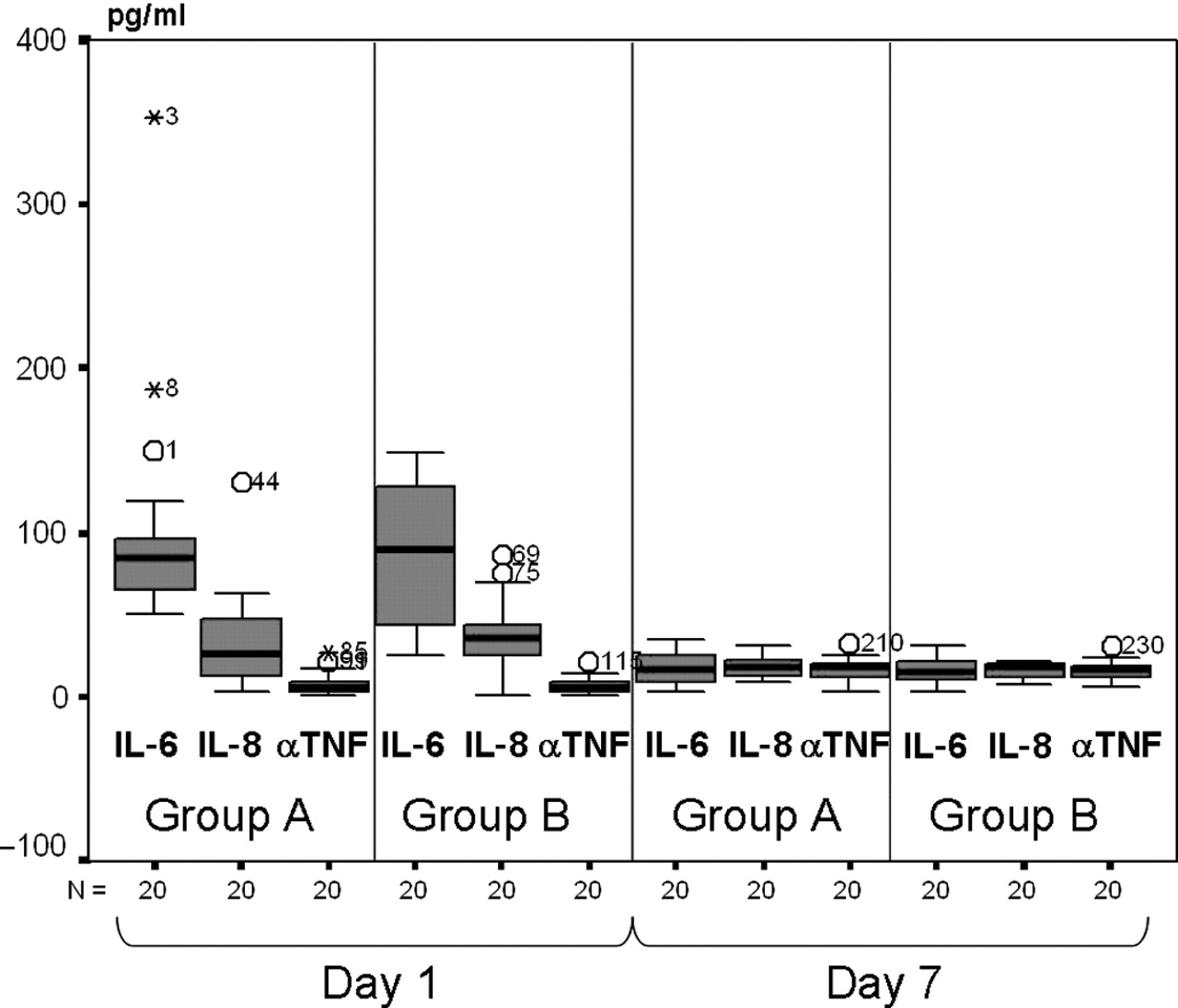
IL6, IL8 and TNFα levels were similar between the two groups at any time of the study (p=not significant), and showed a similar pattern during the study in both groups with a decreasing level of the cytokines (p=not significant) (figure 1).

{kind=link}
Box plot representation of serum cytokines levels (pg/ml) in group A (nasal continuous positive airway pressure (NCPAP)) and group B (bi-level NCPAP) at birth (day 1) and at day 7 of the study.
Respiratory outcomes are shown in table 3: respiratory support and O2 dependency lasted significantly longer in group A; no differences were noted in incidences of reintubation (3/20 vs 2/20), INSURE practice (5/20 vs 5/20), total number of mean surfactant doses (1 vs 1), IVH ≥1 (2/20 vs 0/20), pneumothorax (1/20 vs 0/20) in group A vs group B, respectively. No BPD (O2 dependency at 28 days), chronic lung disease (CLD; O2 dependency at 36 weeks), periventricular leukomalacia (PVL), necrotising enterocolitis (NEC) or deaths occurred in the two groups.
Respiratory and clinical outcomes in group A and group B (values expressed as mean±SD)
There were not significant differences in the incidence of mortality rate, PVL, IVH, retinopathy of prematurity (ROP), BPD and CLD between the two groups.
Discussion
There is evidence that some non-invasive respiratory supports reduce the rate of reintubation of very premature infants. There is some non-conclusive evidence that non-invasive respiratory support may be useful in the treatment of apnoea. There is limited evidence that these supports may be used as a primary approach to moderate RDS in its acute phase; an international European randomised controlled trial that will give useful indications about the optimal respiratory strategy to adopt in high-risk premature infants is still ongoing.20,–,24
Our choice of settings was empirical, since the effects of different settings during bi-level NCPAP on the success of this respiratory support has not been investigated yet and most studies do not mention the applied parameters (in particular Thigh). There is no evidence that a longer Thigh may optimise lung recruitment, but it is obviously preferred to continuous flow systems.
Nevertheless, in the bi-level NCPAP group we set the Thigh at 0.5–0.7 s, the minimal time considered effective to allow the newborn to complete at least one inspiration at the upper CPAP level. We set the pressure exchange rate at 30/min to increase minute ventilation, with a reduced risk of lung derecruitment.
Since we investigated the differences between two different variable flow system supports, we compared a mean airway pressure level of 6 cm H2O (in group A (NCPAP)) to a mean airway pressure level of 6 cm H2O (in group B (bi-level NCPAP)); this choice seemed to make the two groups comparable.
We evaluated the inflammatory response in preterm infants with acute moderate RDS undergoing two different non-invasive ventilatory supports, by monitoring serum levels of proinflammatory cytokines (IL6, IL8, TNFα). Obviously, this forced us to perform a very careful study of medical history and to perform an early exclusion of cases in which sepsis or maternal infection were diagnosed. The important roles of TNFα, IL1β (as representative cytokines of the first line immune response), IL6 and IL8 (as second line and thus suggested to be more consistently elevated) has been demonstrated in the pathogenesis of inflammation and infection.6,–,11 Plasma levels of TNFα, IL1β, IL6 and IL8 (the most extensively studied cytokine in neonates) seem to be the result of the endogenous neonatal production, and have been demonstrated to predict neonatal early onset sepsis with a high sensitivity and specificity.12,–,15 IL6 (early peak) seems to be an important marker of BPD, while TNFα (later peak) may play a critical role in maintaining chronic inflammation in BPD.
Our study demonstrates that the use of bi-level NCPAP allows for an adequate gas exchange inducing the same changes in the cytokine levels as in NCPAP ventilation.
Even if it was not the primary endpoint of our study, the different duration of ventilatory support between the two modalities is an important clinical result, since it implies the achievement of a precocious clinical stability for premature infants.
We speculate that respiratory support and O2 dependency probably lasted significantly longer in the NCPAP group because of less stable lung recruitment: bi-level NCPAP might be more efficacious in stabilising the airways and in reaching and maintaining the optimal FRC, allowing spontaneous breathing on two different levels of CPAP. This study was not designed with this endpoint in mind and we do not have data to confirm this theory. The significantly precocious time of discharge in the bi-level NCPAP group may be attributed to a more rapid achievement of stable clinical condition in these babies.
Limitations of this study include the small number of patients and the lack of blinding of the NICU staff, so further studies will be required to confirm our results; the laboratory staff who checked the cytokine levels were blinded to the ventilatory strategy used, however, and the results communicated at the end of the study.
From our clinical preliminary observations, we hypothesise that a Thigh of 1 s would better support infant breathing, and this is now under study in a new cohort of infants.
In conclusion, this new ventilatory strategy seems to be efficacious when used in preterm infants in the acute phase of moderate RDS. However, further investigations are necessary to establish the best strategy and appropriate ventilator parameters that ensure safety and efficiency.
Acknowledgments
The authors would like to thank the neonatal nurse staff at V.Buzzi Children's Hospital for their support and skilled care of our patients.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the V.Buzzi Children's Hospital Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Patient consent Parental consent obtained.