Article Text

Abstract
Background: Although a low socioeconomic status has consistently been associated with an increased risk of preterm birth, little is known about the pathways through which socioeconomic disadvantage influences preterm birth.
Aim: To examine mechanisms that might underlie the association between the educational level of pregnant women as an indicator of socioeconomic status, and preterm birth.
Methods: The study was nested in a population-based cohort study in the Netherlands. Information was available for 3830 pregnant women of Dutch origin.
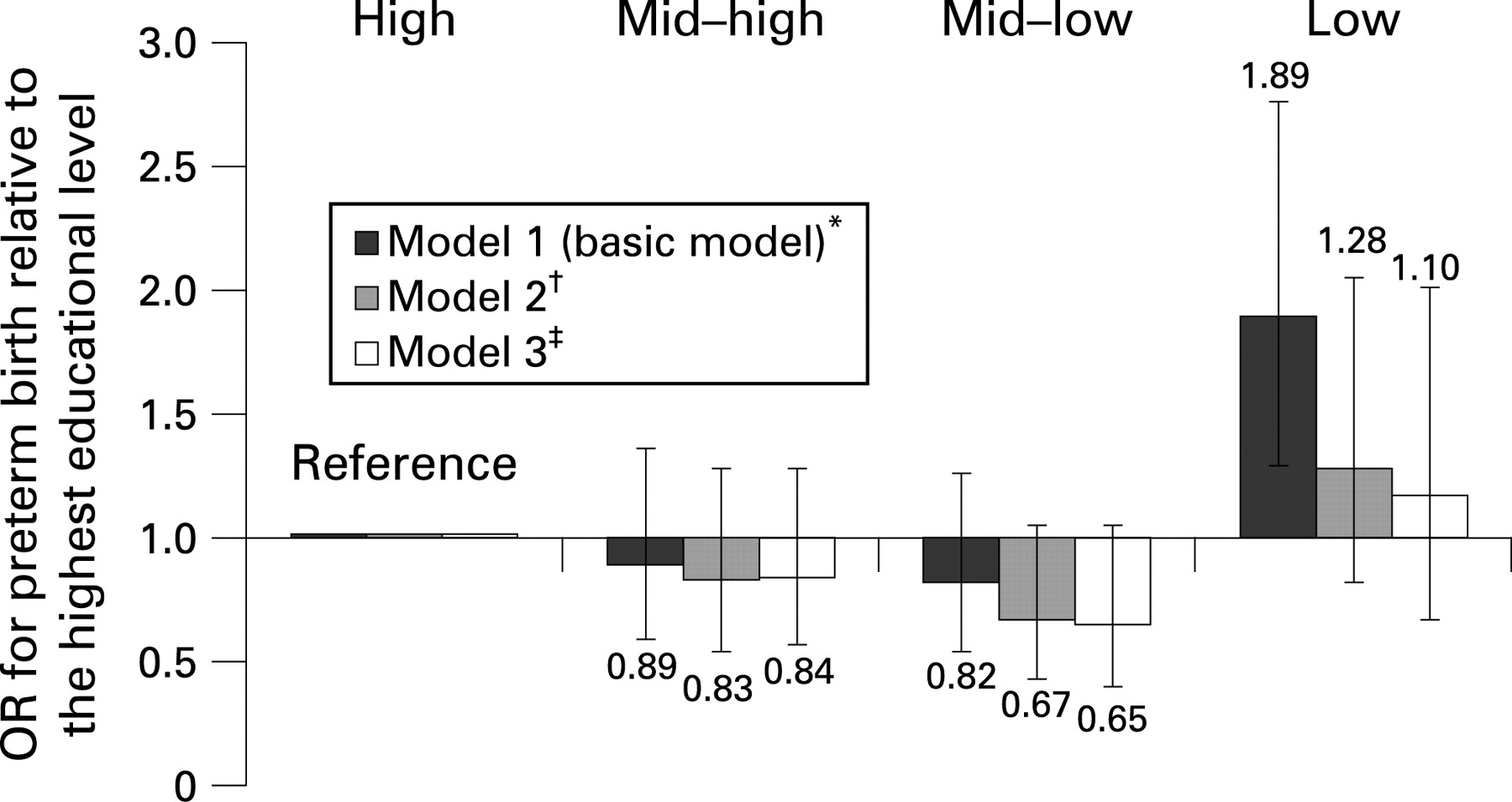
Findings: The lowest-educated pregnant women had a statistically significant higher risk of preterm birth (odds ratio (OR) = 1.89 (95% CI 1.28 to 2.80)) than the highest educated women. This increased OR was reduced by up to 22% after separate adjustment for age, height, preeclampsia, intrauterine growth restriction, financial concerns, long-lasting difficulties, psychopathology, smoking habits, alcohol consumption, and body mass index (BMI) of the pregnant women. Joint adjustment for these variables resulted in a reduction of 89% of the increased risk of preterm birth among low-educated pregnant women (fully adjusted OR = 1.10 (95% CI 0.66 to 1.84)).
Conclusions: Pregnant women with a low educational level have a nearly twofold higher risk of preterm birth than women with a high educational level. This elevated risk could largely be explained by pregnancy characteristics, indicators of psychosocial well-being, and lifestyle habits. Apparently, educational inequalities in preterm birth go together with an accumulation of multiple adverse circumstances among women with a low education. A number of explanatory mechanisms unravelled in the present study seem to be modifiable by intervention programmes.
Statistics from Altmetric.com
Preterm birth is strongly related to perinatal mortality.1 2 Furthermore, infants born preterm are vulnerable to complications and morbidity in the neonatal phase as well as in later life.1 3 Research on socioeconomic inequalities in birth outcome across different industrialised countries has indicated that low educational level, low occupational status, and high deprivation scores are associated with an increased risk of preterm birth.4–10 Only few studies found no relation between socioeconomic status (SES) and preterm birth.11 12 Despite the abundance of studies describing SES inequalities in preterm birth, little research has evaluated the pathways through which socioeconomic disadvantage influences preterm birth: either no possible explanatory variables were taken into account8–10 or only a few, such as age, height, and smoking habits of pregnant women.4–6 However, these few variables could not fully explain the SES variation in preterm birth.4–6 In two recent reviews it is hypothesised that psychosocial risk factors and unhealthy lifestyle habits may explain part of the SES inequalities in preterm birth, since these variables are both determinants of preterm birth and more prevalent among women in the lower SES strata.13 14 This hypothesis has not yet been verified.
In the present study we applied educational level of pregnant women as an indicator of SES. Our objective was to examine the association between education and preterm birth. Additionally, we explored whether the educational inequalities in preterm birth could be explained by pregnancy characteristics, psychosocial factors, and lifestyle habits. For this, we used data from the Generation R study, a large prospective birth-cohort study. The present study involved ethnic Dutch participants only, as educational inequalities in pregnancy outcome and the related explanatory mechanisms may differ between Dutch women and women with another ethnic background.13 15
METHODS
Design
This study was nested in the Generation R study, a population-based cohort study from fetal life until young adulthood.16 17 All pregnant women living in the study area in Rotterdam, the Netherlands, were informed about the study by healthcare workers (eg, community midwives and obstetricians). In total, 8880 pregnant women of different ethnicities with a delivery date between April 2002 and January 2006 enrolled in the prenatal part of the study (response rate 61%). Sixty-nine per cent of all participants enrolled in early pregnancy (<18 weeks’ gestation).
Population for analysis
Of the 8880 women who enrolled in the Generation R study during pregnancy, those with a Dutch ethnicity were selected for the present study (n = 4057). Participants with missing data on education (n = 21) or gestational age (n = 46) were excluded. We also excluded twin pregnancies (n = 54), as preterm birth rates differ considerably between singleton and multiple births.2 18 Women who enrolled after 25 weeks’ gestation were excluded (n = 106), since pregnancy dating based on ultrasound becomes less reliable as pregnancy proceeds,19 yielding a sample size of 3830 participants. In 8.5% of the 3830 women, the pregnancy was their second or third pregnancy in the study. Since there were no differences in results after exclusion of these pregnancies, they were included in the analyses.
Educational level
The highest attained educational level of the participants was assessed by questionnaire. Following the definition of Statistics Netherlands,20 education was categorised as low (primary school; lower vocational training; intermediate general school; 3 years’ general secondary school); mid–low (>3 years’ general secondary school; intermediate vocational training; 1st-year higher vocational training); mid–high (higher vocational training; Bachelor’s degree); and high (higher academic education; PhD).
Preterm birth
Gestational age was determined by fetal ultrasound examination at the first visit to our research centre. Pregnancy dating curves were constructed using subjects of whom we had both ultrasound examinations <25 weeks’ gestation and reliable information on last menstrual period.21 Subsequently, all pregnancies in our study were dated using these curves; the crown–rump length was used for pregnancy dating up to 65 mm (n = 1351) and biparietal diameter was used for pregnancy dating from 23 mm onwards (n = 2479). This corresponds to 12+5 weeks’ gestation. Information on date of birth was obtained from midwife and hospital registries. Birth was classified as preterm if it occurred <37 weeks’ gestation.
Covariates
The choice of covariates that might explain the association between educational level and preterm birth, was based on the literature on determinants of preterm birth.1 7 13 14
Information on gender, preeclampsia, and intrauterine growth restriction (IUGR) was obtained from midwife and hospital registries. Age, height and weight of the pregnant women were assessed at enrolment. Body mass index (BMI) was calculated (kg/m2). The following covariates were assessed by questionnaire: parity, which we defined as the number of live births the participants previously delivered (0, ⩾1); marital status (married/cohabiting, single motherhood); whether the pregnancy was planned (yes, no); financial concerns (no, some, great); smoking habits during pregnancy (non-smoking, smoked until pregnancy was known, continued smoking); and alcohol consumption in mid- and late pregnancy (non-drinking, <1 drink per week, 1–6 drinks per week, ⩾1 drink per day). Long-lasting difficulties during the year preceding the pregnancy were evaluated with an 12-item checklist.22 We assessed psychopathology using the Brief Symptom Inventory, which consists of 53 positive and negative self-appraisal statements.23 In late pregnancy we asked the participants to report on weekly working hours.
Statistical analyses
The association between educational level of the pregnant women and preterm birth was examined using logistic regression analysis (reference group: highest education). This association adjusted for parity and gender was presented as the basic model (BM). We assessed whether the covariates explained (part of) the differences in risk of preterm birth between the educational groups by separately adding the covariates to the BM. We calculated the percentage change in odds ratios (ORs) per educational category brought about by adding a covariate to the BM (100 × [ORBM – ORextended model]/[1 − ORBM]). Finally, the BM was adjusted for all covariates that led to a change of more than 5% in ORs in the above analyses. We conducted the final analysis with and without the covariates preeclampsia and IUGR, as these covariates are very proximal factors and thereby, the risk of over-controlling emerges.
To substitute missing data on the covariates, multiple imputation (function AregImpute in S-Plus 6.0) was applied, using the relations between the variables in the dataset. Since the procedure was repeated five times, multiple imputation took account of the uncertainty of the imputed values.24 The percentages of missing values per covariate were all below 17%. Complete data were available in 69% of the subjects, 30% of the subjects had less than four missing values on covariates, and 1% had four or more covariates imputed.
The statistical analyses were repeated within the subgroup of women who went into labour spontaneously. We also repeated the analyses within the subgroup of women who provided complete information (complete-case analysis). All statistical analyses were performed using the Statistical Package of Social Sciences version 11.0 for Windows (SPSS Inc, Chicago, Illinois, USA) and S-Plus 6.0 Professional Release 1 (Insightful Corp., Seattle, Washington, USA).
RESULTS
General characteristics
Table 1 shows the general characteristics of the study population per educational level.
The mean age of all pregnant women in the study population was 31.3 years (SD = 4.5). The lowest-educated women were younger (F-test = 192; df = 3; p<0.001) and had higher psychopathology scores (F-test = 54; df = 3; p<0.001) than women with the highest education. Compared to the highest-educated pregnant women, the lowest-educated women had an increased risk of preterm birth (OR = 1.89 (95% CI 1.28 to 2.80)).
Covariates
Table 2 illustrates the explanatory effect of several covariates on the association between educational level of the pregnant women and preterm birth. Separate addition of marital status, pregnancy planning, and working hours to the basic model resulted in changes in ORs for preterm birth of less than 5%. Therefore, these covariates were not included in further analyses. Separate addition of participants’ age, height, preeclampsia, IUGR, financial concerns, long-lasting difficulties, psychopathology, smoking habits, alcohol consumption, and BMI to the basic model, substantially (ie, 5%–22%) decreased the ORs of preterm birth in the various educational subgroups as compared to the highest education. The most marked decreases in OR were observed in the lowest-educated women. For instance, long-lasting difficulties accounted for 9% of the increased OR for preterm birth in the lowest-educational group, while this covariate decreased the ORs by 1% in mid–high- and 3% in mid–low-educated women.
Table 3 and fig 1 show the association of educational level with preterm birth after adjustment for all covariates that independently led to a significant change in the separate analyses. Full adjustment for the covariates resulted in a reduction of 89% of the increased risk of preterm birth among low-educated women (parity and gender adjusted OR: 1.89 (95% CI 1.28 to 2.80); fully adjusted OR: 1.10 (95% CI 0.66 to 1.84)). In none of the educational groups the fully adjusted ORs were statistically significant. The difference between the models with and without the covariates preeclampsia and IUGR was marginal for the mid–high- and mid–low-educated women, while among the low-educated women these covariates led to a further reduction of the OR on top of the other covariates (reduction model 2: 69%; reduction model 3: 89%).

{kind=link}
The association between educational level and preterm birth in the subgroup of women who went into labour spontaneously (n = 2474) was comparable to the results of the whole study population (n = 3830). The complete-case sample (n = 2642) consisted of 74% of the high-educated, 75% of the mid–high-educated, 66% of the mid–low-educated, and of 55% of the low-educated women of the initial study population. Preterm birth was less prevalent in the complete-case sample (4.1%) than in the total study population (4.8%). Moreover, the risk of preterm birth in the lowest-educated women (OR = 1.68 (95% CI 0.98 to 2.86)) was smaller in the complete-case sample than in the total study population. In the fully adjusted model, the OR attenuated to 0.80 (95% CI 0.40 to 1.61).
DISCUSSION
This prospective population-based study showed that women with a low-educational level had a nearly twofold higher risk of preterm birth compared to women with a high-educational level. This elevated risk was roughly explained by an unfavourable combination of pregnancy characteristics, psychosocial well-being, and lifestyle habits, that was present in lower-educated women.
In our study, only the subgroup of women with the lowest-educational level had a significantly increased risk for preterm birth as compared to the subgroup of high-educated women. Previous studies using other indicators of SES reported an inverse linear trend between SES level and risk of preterm birth.4–10 Future studies, preferably with larger samples, should verify whether only very low-educated women are at risk for preterm birth or whether our findings occurred by chance. The magnitude of the OR for preterm birth among low- versus high-educated women compares well with earlier findings from Western countries.4–10 For instance, Peacock et al also reported the prevalence of preterm birth in the UK roughly to be twice as high in the lower SES strata as compared to high SES.9
Explanation of risk of preterm birth
The current study explained a substantial amount, that is, 89% of the elevated risk of preterm birth among the lowest-educated women. This was accomplished by including a comprehensive set of potential explanatory factors, namely adverse pregnancy characteristics, psychosocial variables and lifestyle factors, that were chosen on the basis of existing knowledge.1 7 13 14 Besides an on-average younger age and shorter height, women with a low SES seem to have an accumulation of adverse circumstances, especially regarding psychosocial stress and unhealthy lifestyle habits, that turned out to be associated with their increased risk of preterm birth. Previous studies on SES inequalities in preterm birth explained at best 65% of the increased risk among lower SES women. However, in these studies only a limited number of explanatory factors was included.4–7
Pregnancy characteristics
In our study, a relatively high prevalence of preeclampsia and IUGR was found among lower-educated women. Since both preeclampsia and IUGR are highly associated with and often the direct cause of preterm birth, these medical conditions explained part of the increased risk of preterm birth among low-educated women. Preterm birth due to preeclampsia or IUGR can occur spontaneously or may be induced to reduce health risks in both mother and child.25 26 The fully adjusted analyses with and without preeclampsia and IUGR indicated that, only among the lowest-educated women, these two conditions explained an additional part of the elevated risk of preterm birth.
Indicators of psychosocial stress
Psychosocial factors, such as financial concerns, “long-lasting difficulties”, and psychopathology of the pregnant women, explained a substantial part of the increased risk of preterm birth among low-educated women. This finding is in line with theories on the effects of prenatal stress, in which psychosocial stress is hypothesised to be associated with a relatively higher risk of preterm birth through specific patterns of a pregnant woman’s physiological and hormonal response to stress.27 28
Lifestyle habits
With regard to BMI, a factor that we consider as an indicator of physical activity and diet, both overweight (BMI >25) and especially thinness (BMI <18) are well-established risk factors for preterm birth.13 29 30 In our study, BMI clearly contributed to the explanation of educational differences in risk of preterm birth. We hypothesise that the impact of overweight on preterm birth among low-educated women is larger than the impact of thinness, since overweight is much more prevalent in this educational subgroup than thinness.
We showed that continuation of alcohol consumption during pregnancy, which is relatively less common among women with low education as compared to higher-educated women, also explained a considerable part of the educational inequalities in preterm birth. It is hypothesised that low to moderate alcohol consumption during pregnancy may be genuinely beneficial, although the effects may also be explained by the “healthy drinker effect”, in which women with a poor obstetric history are more likely to abstain from drinking.31 Clearly, further research is required to test these hypotheses.
Strengths and limitations
The strengths of the present study are the large number of participating pregnant women with different levels of education, its prospective population-based design and the detailed information on numerous relevant covariates. Another strong point is that gestational duration was established by fetal ultrasound examination, as using the last menstrual period has several limitations, including the large number of women who do not know the exact date of their last menstrual period or have irregular menstrual cycles.32 A final strength of the study is the thorough missing values procedure that was applied. We decided to impute missing data instead of excluding those with missing values, as multiple imputation has the benefit of circumventing selection mechanisms involved in missing values, namely that data were more complete in higher-educated women and among those having a term delivery. Moreover, using multiple imputation instead of complete case analysis also increased statistical power due to a larger study population.
Some methodological issues need to be considered. The participants of the Generation R cohort represent a selection towards a somewhat more healthy population.17 33 Additionally, our study was limited by the availability of covariates, for example, we did not assess the influence of pregnancy interval, dietary intake, bacterial vaginosis, and other stressful circumstances than the ones included. These factors potentially contribute to the explanation of educational inequalities in preterm birth. Finally, it is possible that different educational groups are characterised by different lifestyles and behaviours in various societies, which for instance may be the case regarding alcohol consumption during pregnancy. Therefore, some caution is needed when generalising our results to other populations.
Conclusions
Given the nearly twofold higher risk of preterm birth among low-educated women and the associated medical consequences in the neonatal phase as well as in later life, it is important to invest in policies aimed at reducing educational inequalities in preterm birth.
Even though risk factors for preterm birth among low-educated women may not be easily amendable, there might be opportunities that are not yet applied effectively. Several of the explanatory factors identified in this study, such as young age, stressful circumstances, smoking habits and overweight, are modifiable by up-to-date interventions.34–37 Initiation of preventive interventions during pregnancy may be too late. Therefore, the most effective strategy for tackling educational inequalities in preterm birth is probably by nesting these programmes in preconception care.38
What is already known on this topic
Low socioeconomic status has often been associated with an elevated risk of preterm birth.
A pregnant woman’s age and smoking habits explain part of the association between socioeconomic status and preterm birth, but these factors cannot explain the whole association.
What this study adds
Pregnant women with a low socioeconomic status (SES), as indicated by their educational level, had a nearly twofold higher risk of preterm birth than pregnant women with a high SES.
Educational inequalities in preterm birth resulted from an unfavourable combination of various pregnancy characteristics, psychosocial factors, and lifestyle habits, that was present in lower-educated women.
Acknowledgments
The Generation R study is conducted by the Erasmus MC — University Medical Center Rotterdam in close collaboration with the Erasmus University Rotterdam School of Law and Faculty of Social Sciences; the Municipal Health Service Rotterdam area, Rotterdam; the Rotterdam Homecare Foundation, Rotterdam; and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR), Rotterdam. We gratefully acknowledge the contribution of the participating pregnant women and their partners, and also of general practitioners, hospitals, midwives and pharmacies in Rotterdam.
The first phase of the Generation R study is made possible by financial support from the Erasmus MC – University Medical Center Rotterdam, Erasmus University Rotterdam, and the Netherlands Organization for Health Research and Development (ZonMW).
REFERENCES
Footnotes
None.
The Medical Ethical Committee of the Erasmus Medical Center, Rotterdam, has approved the study.
Written informed consent was obtained from all participants.
The present study was supported by an additional grant from the Netherlands Organization for Health Research and Development (ZonMW “Geestkracht” program 10.000.1003).
Linked Articles
- Fantoms