Article Text

Abstract
Background: B-type natriuretic peptide (BNP) is a marker for ventricular dysfunction secreted as a pre-prohormone, pro-B-type natriuretic peptide (proBNP), and cleaved into BNP and a biologically inactive fragment, N-terminal pro-B-type natriuretic peptide (NT-proBNP). Little is known about the clinical usefulness of NT-proBNP in preterm infants.
Objective: To evaluate the usefulness of plasma NT-proBNP in diagnosing haemodynamically significant patent ductus arteriosus (hsPDA) in neonates and examine some factors that might affect this.
Methods: Infants born at <34 weeks’ gestational age (GA) and <2 kg birth weight (BW) were prospectively enrolled within 6–12 hours of birth. Plasma NT-proBNP levels were measured on days 1, 3, 5 and 10 with simultaneous echocardiography done to detect hsPDA and assess ventricular function. Significant PDA was diagnosed by large ductal flow with left to right shunt on colour Doppler, measuring >1.6 mm on two-dimensional echocardiography, along with clinical features of PDA.
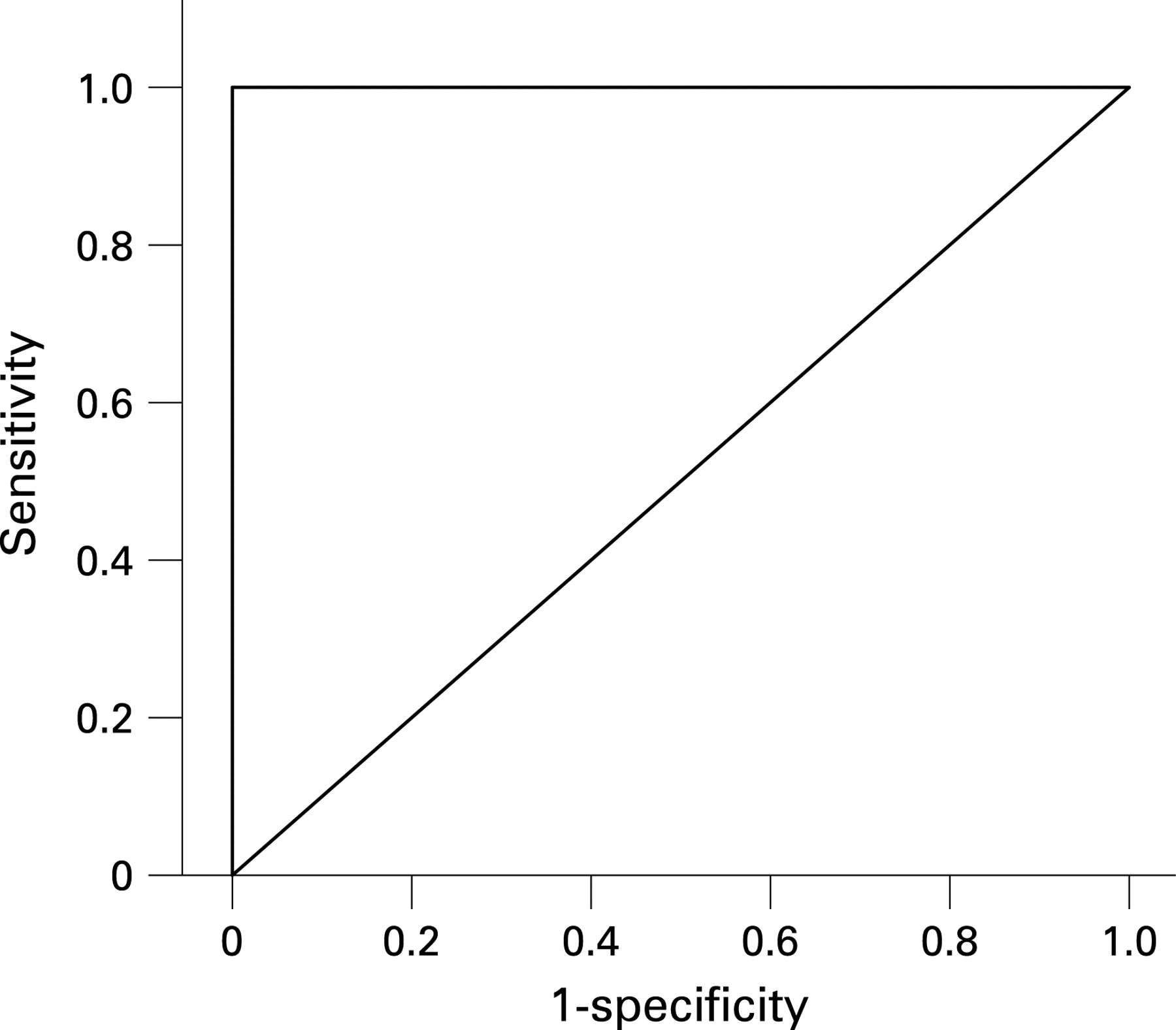
Results: Forty-nine infants were analysed. Median GA was 30 weeks (range 24–33) and median BW 1220 g (range 550–1950). Eighteen infants with hsPDA had higher day 3 plasma NT-proBNP values (median 32 907 pg/ml; range 11 396–127 155) (p<0.001) than controls (median 3147 pg/ml; range 521–10 343). Infants who developed sepsis had higher day 10 plasma NT-proBNP levels. Area under receiver operator characteristic curve for detection of hsPDA, by day 3 NT-proBNP value, was significant 0.978 (95% CI 0.930 to 1.026). NT-proBNP was predictive of hsPDA (sensitivity 100%; specificity 95%) at a cut-off value of 11 395 pg/ml.
Conclusion: Plasma NT-proBNP level on day 3 is a good marker for hsPDA in preterm infants. Serial measurements of NT-proBNP may be useful in assessing the clinical course of PDA.
Statistics from Altmetric.com
B (brain)-type natriuretic peptide (BNP) is synthesised and released almost exclusively by ventricular myocardium in response to pressure or volume overload. BNP acts as a vasodilator and has diuretic and natriuretic properties, suppressing the effects of the renin–angiotensin–aldosterone system. The measurement of plasma BNP levels is used in adult patients in the diagnosis and management of congestive heart failure.1 2 BNP is a highly sensitive prognostic indicator of outcome in patients with ventricular end-diastolic dysfunction.2–4
BNP is synthesised as a pre-prohormone containing 134 amino acids; it is cleaved to proBNP (108 amino acids). ProBNP is further cleaved into the biologically active BNP, which contains 32 amino acids, with a half-life of 20 minutes, and the inactive fragment, N-terminal proBNP (NT-proBNP),1 which has a longer half-life of 60 minutes.5
BNP and its inactive fragment, NT-proBNP, can be measured rapidly and accurately at the point of care.2 3 A few studies have reported on the application of measuring plasma BNP levels in the neonatal population,6 7 mainly focusing on its use in the diagnosis of haemodynamically significant patent ductus arteriosus (hsPDA)7–11; little is known about the clinical usefulness of its inactive fragment, NT-proBNP, in this patient population. More recently, plasma NT-proBNP concentrations had been assessed in children with congestive heart failure.7
Rapid and accurate determination of the presence of hsPDA is important as its presence is a major cause of morbidity in preterm infants.12 13 PDA is diagnosed clinically by the presence of a systolic murmur, a hyperactive praecordium, and full or bounding pulses with confirmation by echocardiography. These signs are detected only after the left to right shunt through the duct has been significant for some days.14 15 Although echocardiography is the preferred method for the assessment of PDA,14 15 it has considerable intra- and interobserver variability; the criteria for assessment of the degree of shunting through an hsPDA are not well defined.14 Many neonatal units do not have easy access to echocardiography for assessment of PDA.
We evaluated the clinical usefulness of the measurement of plasma NT-proBNP levels in preterm infants. We examined the value of repeated measurement of plasma levels of NT-proBNP to identify the best cut-off level of NT-proBNP for predicting hsPDA.
METHODS
This prospective observational study was approved by the Ethics and Research Committee of Rotunda Hospital, Dublin. Written and signed informed parental consent was obtained before enrolment of each baby. Preterm infants who were <34 weeks’ gestational age (GA), and <2.0 kg birth weight (BW) were eligible for entry into the study. Infants were enrolled within 6–12 hours of birth. Exclusion criteria included congenital anomalies, including congenital heart disease other than PDA. Enrolment was limited by the ability to obtain consent and availability of the principal investigator to collect blood samples and perform echocardiography. Blood samples for NT-proBNP measurement were collected either from indwelling arterial catheters or peripheral veins together with routine blood samples to avoid extra needle sticks and excessive blood sampling.
NT-proBNP and BNP pilot study
A pilot study of 10 preterm infants (<34 weeks’ GA, <2.0 kg BW) was undertaken to compare the BNP (Architect; Abbott Laboratories, Illinois, USA) and NT-proBNP (Elecsys; Roche Diagnostics Ltd, UK) assays. Blood samples were taken on days 1, 3 and 5 of life. Sixty blood samples (30 paired samples) were analysed. The Abbott Architect BNP assay required an EDTA blood sample while the Roche NT-proBNP assay required a lithium heparin sample.
Arterial and venous blood samples were obtained simultaneously from seven infants to determine whether there was any difference in arterial and venous plasma NT-proBNP levels.
There was no significant difference between arterial plasma NT-proBNP (median 9045 pg/ml; range 2028–210 689) and venous plasma NT-proBNP (median 9836 pg/ml; range 1960–214 573) levels (p = 0.176).
The interassay coefficient of variation for BNP was 4.4% at 118 pg/ml and for NT-proBNP was 0.81% at 2120 pg/ml. There was a good correlation between plasma NT-proBNP and BNP measurement (r = 0.96, p<0.001); the former assay was used for the main study principally because it could be assayed on the sample type required for “routine” biochemistry, therefore reducing the total amount of blood drawn. This fulfilled the ethics committee requirement for minimal blood sampling.
NT-proBNP assay
Blood samples were collected on days 1, 3, 5 and 10 of life for plasma NT-proBNP measurement. Blood was taken from indwelling umbilical arterial catheters or peripheral vein, collected into lithium heparin tubes and sent immediately to the laboratory for centrifugation. Plasma was aliquoted and stored at −20°C until analysed in batches. An electrochemiluminescence immunoassay was performed on a Roche Elecsys 2010 analyser according to the manufacturer’s instruction. The assay range was 5–35 000 pg/ml; higher values were obtained by dilution with Roche Elecsys universal diluent.
Echocardiography
Two-dimensional echocardiography was performed on all infants within 1 hour of blood sampling for assessment of PDA and to rule out congenital heart disease. A Siemens Sonoline G60S ultrasound machine with curvilinear 8 MHz transducer was used (Siemens Medical Solutions USA Inc, PA, USA). Echocardiography was done on days 1, 3, 5 and 10 of life by one investigator (IF-O) to avoid interobserver variability.
Left ventricular shortening fraction was assessed on M-mode measurements by measuring the percentage change in left ventricular diameter during systole. A parasternal long-axis view was obtained with the M-mode cursor at the level of the mitral valve, perpendicular to the right ventricle (anteriorly), interventricular septum and left ventricle. Left ventricular end-diastolic function diameter and left ventricular end-systolic diameter were measured with continuous electrocardiography. The shortening fraction was automatically calculated on the ultrasound machine.
A significant PDA was diagnosed by large ductal flow with left to right shunt on colour Doppler which measured at least 1.6 mm on two-dimensional echocardiography with retrograde flow in the descending aorta.14–16 The infants with hsPDA were treated with either six doses of indometacin,17 or three doses of ibuprofen18; treatment was carried out between days 3 and 10 of life in both groups.
The choice of modality of treatment of hsPDA was based on the clinical status of the infant and clinician preference. The less stable infants or those with suspected bowel disease were treated with ibuprofen and others were given a longer course of indometacin.19
Statistical analysis
Analysis was performed using SPSS, version 15 (SPSS Inc, Chicago, Illinois, USA). The Mann–Whitney rank-sum test was used to calculate the differences between the groups where applicable. A Wilcoxon signed ranks test was used for comparison of arterial and venous NT-proBNP plasma levels. Multiple regression analysis, using beta (β) weights was performed to determine the effect of gestational age, prolonged rupture of membranes, use of inotropes, presence of sepsis and significant PDA as independent variables, on the plasma levels of NT-proBNP on days 1, 3, 5 and 10. A p value of <0.05 was considered significant. Receiver operator characteristic (ROC) analysis was performed to determine the best cut-off values of plasma NT-proBNP levels for the detection of significant PDA.
RESULTS
Over a 9-month period, 52 preterm infants (<34 weeks’ GA, <2 kg BW) were prospectively enrolled into the study. Three infants were excluded from the data analysis because full data were not available. The 49 infants (32 male, 17 female) analysed had a median GA of 30 weeks (range 24–33) and median BW 1220 g (range 550–1950).
The infants with hsPDA were generally of lower birth weight and younger gestational age (median BW 1000 g, median GA 26 weeks) than the “non-PDA” infants (median BW 1420 g, median GA 30 weeks).
Plasma NT-proBNP levels were high on day 1 of life and showed a decline from day 3 to day 10 of life except in those infants with significant hsPDA or those who developed culture-proven sepsis (fig 1).

Of the 49 infants, 31 had no hsPDA. Within this group 14 infants demonstrated a progressive fall in plasma NT-proBNP from day 1 to day 10. Fifteen demonstrated an initial fall and then a subsequent rise in plasma NT-proBNP by day 10. On review of the clinical records of this latter group, all infants had late-onset sepsis between day 8 and day 12 of life; plasma NT-proBNP levels were significantly higher (p<0.01) than in the non-septic group on day 10. No infants had culture-proven sepsis between days 3 and 5 of life. Two infants had congenital infections and their plasma NT-proBNP levels were particularly high on day one (fig 1) and subsequently fell from day 3 to day 10 of life.
Eighteen infants had hsPDA. In this group, plasma NT-proBNP levels were significantly higher on day 3 of life than in those with no hsPDA and no sepsis (p<0.001) (fig 1).
Table 1 shows the multiple regression analyses studying the effect of gestational age, prolonged rupture of membranes, use of inotropes, presence of sepsis and significant PDA as independent variables on plasma levels of NT-proBNP on days 1, 3, 5 and 10 of life. R is the multiple correlation coefficient between the independent variables and NT-proBNP. R2 is the proportion of the variation in NT-proBNP explained by the model.
The analyses showed that the NT-proBNP level was affected by gestational age on day 1 of life, with the level being higher in the more premature infants. (β = −0.495; p = 0.013); however, a value of R2 = 0.162 suggests that none of the independent variables influence NT-proBNP levels greatly. By day 3 of life, plasma NT-proBNP levels were significantly higher in infants with hsPDA (β = 0.583; p<0.001, R2 = 0.558), while late-onset sepsis was a significant predictor of high levels of NT-proBNP on day 10 of life (β = 0.417; p = 0.002).
The area under the ROC curve for the detection of PDA was significant 0.978 (95% CI 0.930 to 1.026). The measurement of plasma NT-proBNP level on day 3 of life was a highly sensitive predictor of hsPDA (sensitivity 100%; specificity 95%) at a cut-off value of 11 395 pg/ml (fig 2).
{kind=link}
{kind=link}
Left ventricular shortening fraction (LVSF) generally improved over the duration of the study, with an increase in LVSF from day 1 to day 10 of life. There was no significant difference in the LVSF on day 10 between those infants with sepsis and those with no evidence of sepsis (median LVSF in the septic group 33.3%; range 29–40%, median LVSF in non-septic group 32.0%; range 30–40%; p = 0.905).
What is already known on this topic
Natriuretic peptides (ANP and BNP) are raised in infants with congenital heart disease and myocardial dysfunction.
A strong correlation exists between high plasma levels of BNP and significant PDA.
DISCUSSION
PDA is a significant cause of morbidity in very preterm infants with complications such as persistent pulmonary hypertension,12 pulmonary haemorrhages,13 low systemic blood flows and intraventricular haemorrhages.20 21 Early diagnosis of hsPDA allows for earlier treatment and a probable reduction of morbidity in this group.
What this study adds
NT-proBNP has a significant diagnostic value in patent ductus arteriosus (PDA).
The diagnostic cut-off value of NT-proBNP assay for haemodynamically significant PDA was determined.
Sepsis is associated with raised plasma NT-proBNP levels.
A strong correlation between plasma levels of atrial natriuretic peptide (ANP) and PDA in preterm infants was first described by Andersson et al.22 This finding was confirmed by other studies.23 In a subsequent report by Puddy et al, the presence of hsPDA was associated with markedly increased levels of BNP in extremely preterm infants.10
We measured plasma NT-proBNP levels in preterm infants during the first 10 days of life. On the third day of life, plasma NT-proBNP levels were significantly higher in infants with hsPDA than in those without hsPDA in the absence of sepsis. Our results were similar to those found in previous studies,9 10 23 24 in which it had been suggested that the measurement of plasma BNP levels is a useful diagnostic marker of hsPDA requiring medical or surgical intervention.
We have demonstrated that by the third day of life, using the ROC curve, plasma NT-proBNP levels greater than 11 395 pg/ml are strongly predictive of significant PDA, requiring intervention (sensitivity 100%, specificity 95%). This finding also suggests that serial plasma NT-proBNP measurements may be useful in the management of hsPDA10 23 as a complementary tool to echocardiography or as an adjunct to clinical examination, where regular echocardiography expertise is not available.
This study also showed that in those patients with sepsis, plasma NT-proBNP levels are significantly higher on day 10 of life than in those with no hsPDA and no sepsis. This finding is similar to that in a study by Fried et al,25 in which there were raised NT-proBNP levels in a cohort of older children with sepsis. Therefore, NT-proBNP levels need to be interpreted with caution when PDA and sepsis coexist.
The high levels of plasma NT-proBNP in the infants with sepsis may be suggestive of other factors beside myocardial dysfunction as a cause of elevation of this peptide levels. Some animal studies and published reports on adults indicate that cytokines may have a role to play in the upregulation of natriuretic peptides synthesis,26 27 as proinflammatory cytokines have been reported to induce production, and possibly stimulate, the release of BNP during sepsis.28–30
CONCLUSION
Plasma NT-proBNP level is a highly sensitive and specific indicator of hsPDA in preterm infants. It can be measured rapidly at the point of care. The measurement of plasma NT-proBNP levels by day 3 of life may be a useful complementary tool, and a possible alternative to repeated echocardiography in the diagnosis and management of PDA in preterm infants, in the absence of sepsis, especially in neonatal units with limited access to echocardiography.
Acknowledgments
We acknowledge the financial support of the Friends of the Rotunda, Dr Claire Collins and Dr Chris McLaughlin for their invaluable help with the statistical analysis and Mr Niall Ward for his help in reviewing the echocardiography. We also acknowledge the support of the nursing staff in the Neonatal Intensive Care Unit at Rotunda Hospital, Dublin for their close monitoring and care of the infants enrolled into the study and of the staff in the Department of Clinical Biochemistry.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Approved by the Ethics and Research Committee of Rotunda Hospital, Dublin, Ireland
Linked Articles
- Fantoms