Article Text

Statistics from Altmetric.com
- functional imaging
- near infrared spectroscopy
- optical tomography
- optical topography
- perinatal brain injury
Optical systems could be valuable tools for assessing cerebral function at the cotside
The newborn brain is vulnerable to a variety of insults with potentially lifelong consequences. As our understanding of the mechanism of brain injury improves and new therapies are developed to prevent or minimise brain injury, new non-invasive methods are required to assess cerebral function at the cotside.
The application of near-infrared spectroscopy (NIRS) for continuous monitoring of cerebral haemodynamics and oxygenation non-invasively was first reported by Jobsis in 1977.1 Since that time NIRS has become an effective research tool for studying infant cerebral haemodynamics and oxygenation.2,3 NIRS exploits the relative transparency of biological tissue to near-infrared light (700–1000 nm), and the wavelength-dependent absorption characteristics of haemoglobin, which vary with oxygenation. By monitoring the intensity of light passing through brain tissue at two or more wavelengths, observed changes in attenuation can be converted into changes in the cerebral concentrations of oxyhaemoglobin and deoxyhaemoglobin.
FUNCTIONAL NIRS
An obvious application of NIRS is the investigation of localised changes in oxyhaemoglobin and deoxyhaemoglobin resulting from functional activation of the cerebral cortex. Increases in local cerebral blood flow (CBF) are manifested by a rise in oxyhaemoglobin and a fall in deoxyhaemoglobin whereas oxygen consumption during activation results in a decrease in oxyhaemoglobin and an increase in deoxyhaemoglobin. The balance between local perfusion and consumption can be investigated with NIRS.
The first functional studies in the newborn with optical techniques used conventional single source-detector systems to measure overall changes in oxygenation over a particular area of the head. Meek et al reported that, in response to a visual stimulus, there was an increase in both oxyhaemoglobin and deoxyhaemoglobin over the occipital lobe.4 This finding was consistent with those of studies in infants using functional MRI and contrasted with the response in adults, in whom the increase in regional perfusion greatly exceeds the increase in local consumption, resulting in an increase in oxyhaemoglobin and decrease in deoxyhaemoglobin.5 The maturation of this response seems to depend on the type of stimulus and the state of wakefulness of the infant as well as their age, and it is currently an area of active research using optical topography.6,7,8,9,10
Bartocci et al investigated the response to olfactory stimuli in the newborn: they found a significant increase in oxyhaemoglobin measured over the frontal cortex in response to colostrum which was inversely related to postnatal age.11 Neonates were also able to differentiate between pleasant and unpleasant odours.12 Recently the haemodynamic response to pain has been investigated using NIRS.13,14 Slater et al found that preterm infants as young as 25 weeks’ gestation show a cortical response following a heel lance. The response was markedly greater in infants who were awake, indicating the importance of behavioural state in the response to pain.
OPTICAL TOPOGRAPHY
The single source-detector pair studies outlined above obtain measurements over a relatively large volume of the brain and are therefore susceptible to inaccuracies in both localisation and quantification of the response. Optical imaging is therefore a natural extension of efforts to address these issues.
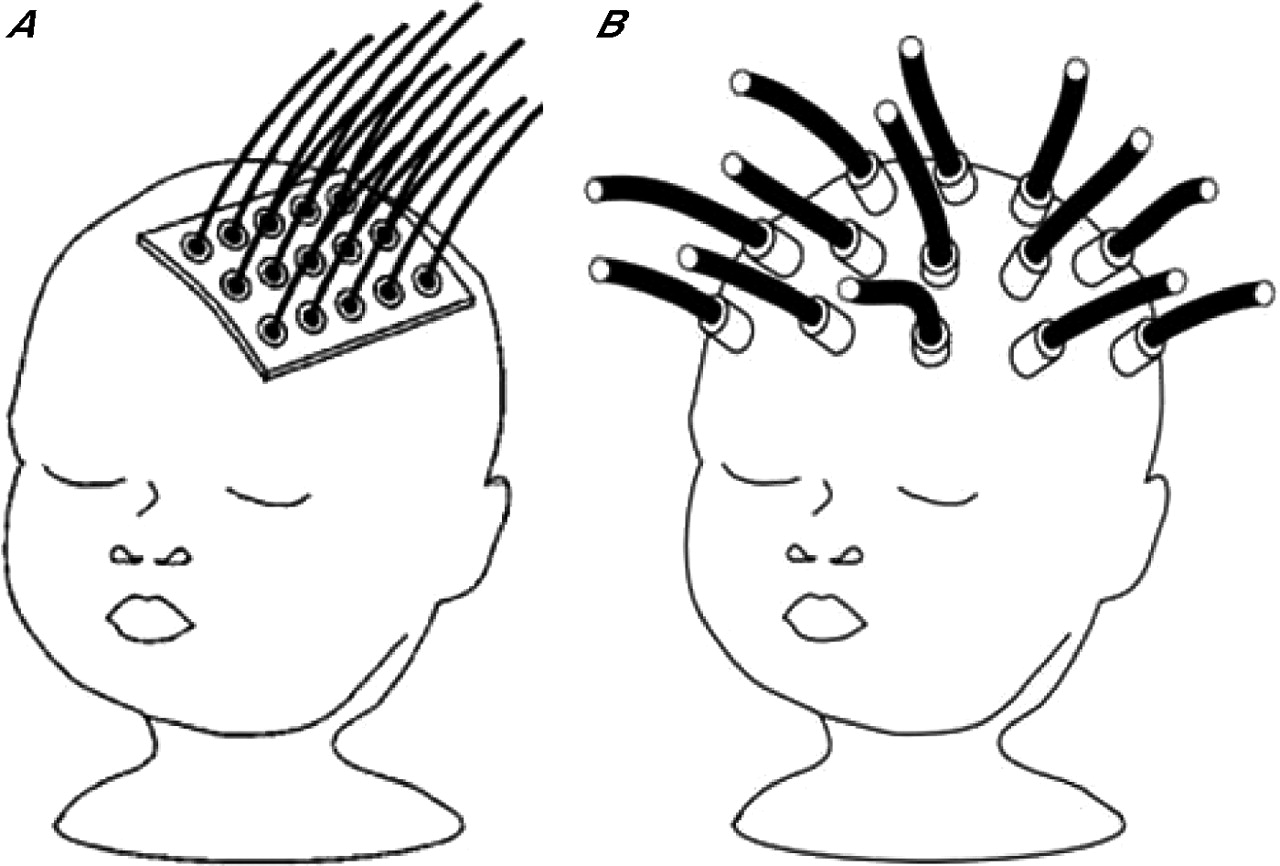
The most straightforward approach is optical topography, which involves acquiring multiple reflectance measurements at small source-detector separations from the surface of the head simultaneously or in rapid succession (fig 1A). By keeping the separations small it is possible to make measurements of rapid changes in haemodynamics associated with functional activation. The penetration of light is limited and so will reflect changes in oxygenation within the cerebral cortex. Several groups have developed custom-built multichannel topographic imaging systems demonstrating the potential of this technique to assess brain function at the cotside.15,16 A commercially available optical topography system (Hitachi ETG-100 optical topography system, Hitachi Medical Corporation, Tokyo, Japan) has been used to investigate the response of neonates to a variety of stimuli, including visual, auditory and somatosensory.8,9,17,18 Pena et al investigated the response of neonates to speech in the first few days of life.18 They found the greatest change in regional blood volume, over the left temporal lobe, was in response to the mother’s speech, compared with “reversed speech”, illustrating the remarkable ability of the human brain for complex neural processing in the first days of life.

(A) Optical topography: the close proximity of optical fibres allow rapid measurements to be obtained from the surface of the brain. (B) Three-dimensional optical tomography: interrogation of the whole volume of the brain is possible by placing optical fibres around the head.
OPTICAL TOMOGRAPHY
In contrast to optical topography, the aim of optical tomography is to obtain a two-dimensional slice or a three-dimensional image of the whole brain. The sensitivity to deep tissue requires measurements across the head, and consequently transmitted light must be interrogated over periods of several seconds or longer for each source to obtain adequate signal (fig 1B). Although this inhibits the display of fast haemodynamic phenomena associated with functional activation, unless averaged over repeated stimuli, this technique is able to obtain information on oxygenation in deeper areas of the brain. The greatest challenge with optical tomography is developing adequate image reconstruction algorithms which can account for the overwhelming scattering of light as it passes through the head.
Static imaging of the infant brain
Two optical tomography systems have been used to date to image the neonatal brain, both based on the measurement of times of flight of photons travelling across the head. The distribution of photon flight times is unique for each source-detector pairing and provides information on the light absorbing and scattering characteristics of the tissue being interrogated.
The first two-dimensional tomographic images of the brain were demonstrated by Benaron et al, who developed an imaging system that measures photon flight times between points arranged around the circumference of the head.19,20 Images representing a transverse slice across the brain were reconstructed using a relatively straightforward backprojection method.21 Scans of infants at a variety of gestational ages successfully showed intracranial haemorrhage and a focal region of low oxygenation after acute stroke.19,20,22 A major drawback of this system was the acknowledged simplicity of the image reconstruction algorithm, which ignored the inherent three-dimensional nature of photon migration in tissues, and the highly heterogeneous nature of the infant head.
To address this issue an iterative non-linear algorithm has been developed at University College London (UCL).23 The algorithm compares the measured data with the simulated data derived from a computer model of the infant brain, and updates the model iteratively until a satisfactory match is achieved. Data have been acquired using a 32-channel time resolved system, designed and built at the Biomedical Optics Research Laboratory, UCL.24 The instrument illuminates the infant head with picosecond pulses of light at two wavelengths (780 nm, 815 nm). Reconstruction images of the internal absorption properties can then be used to generate images of regional cerebral blood volume and regional tissue oxygen saturation.25
Initial studies on premature infants used custom-made, foam-lined, plastic helmets whose dimensions were based on a series of measurements acquired from digital photographs of each infant prior to the study. More recent studies have used an adaptable helmet that can accommodate head sizes of infants from 24 weeks’ gestation to term. A complete dataset can be acquired in 10 minutes. Because the system measures the times of flight of transmitted photons it is less sensitive to movement artefact than conventional near-infrared instruments that only measure transmitted intensity. To date nearly 40 infants have been scanned using the UCL system, with roughly two-thirds of the scans yielding data sufficient for reliable image reconstruction. Failure to obtain images has been due to a variety of factors, such as infant movement, poorly fitting helmet or instrumental instability. The first successful images were reconstructed from a 30-week preterm infant with a large unilateral intraventricular haemorrhage26; this was followed by images obtained on an infant requiring mechanical ventilation. By making appropriate changes to the ventilator settings a unique series of images revealed regional changes in cerebral blood volume and oxygenation.27
Images of regional cerebral blood volume and regional tissue oxygen saturation from healthy infants show considerable heterogeneity, with a reduction in blood volume and oxygenation in the more central regions of the brain.28 This is consistent with studies of regional perfusion using single photon emission computed tomography, demonstrating the vulnerability of the periventricular white matter to hypoxic-ischaemic injury.29 Figure 2 shows coronal slices from three-dimensional images of regional cerebral blood volume and regional tissue oxygen saturation from a preterm infant with a left-sided intraventricular haemorrhage and haemorrhagic parenchymal infarct. A distinct area of desaturated haemoglobin on the left side is seen (10% compared with 62% on the contralateral side). Although more lateral and superficial than the position indicated by the ultrasound scan this is consistent with a resolving blood clot. An ischaemic penumbra surrounding haemorrhagic lesions has been described both in adults and infants and optical tomography will be the ideal tool to explore this concept further.30,31
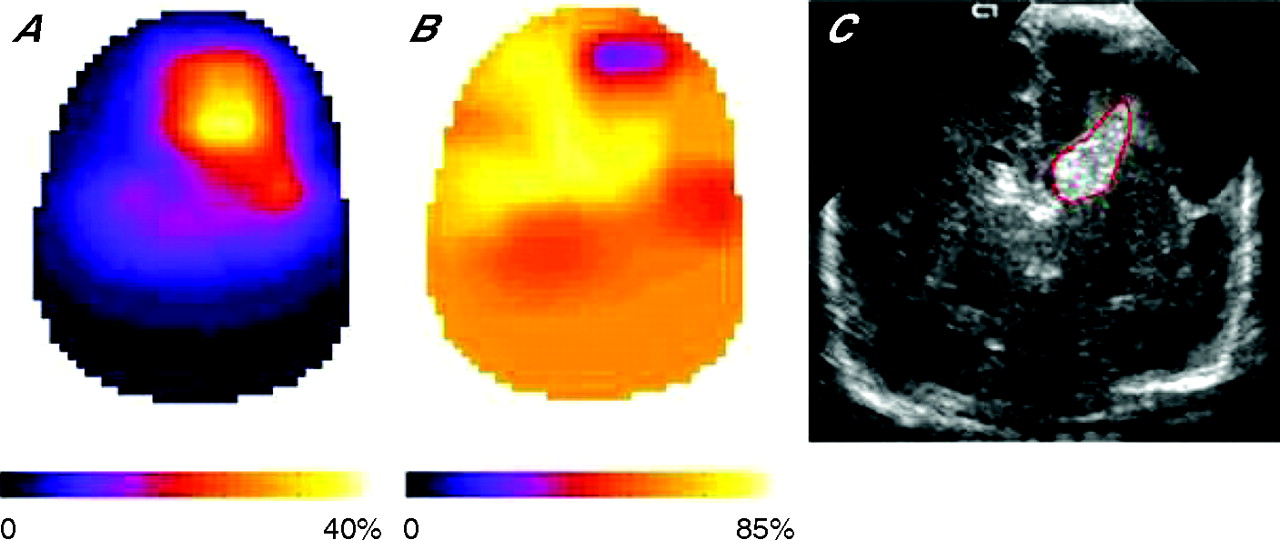
Coronal sections of infant brain images of (A) regional blood volume, (B) regional oxygen saturation and (C) the corresponding ultrasound scan. Reprinted from NeuroImage, 31, Austin T, Gibson AP, Branco G, et al. Three-dimensional optical imaging of blood volume and oxygenation in the preterm brain, figure 5, p. 1431, © 2006, with permission from Elsevier.
Three-dimensional imaging of functional activation
We have recently obtained the first three-dimensional images of the entire neonatal head during motor evoked responses.32 Data were acquired during bilateral passive arm movement, repeated for 12 source positions. A composite image was reconstructed for each infant and demonstrated an increase in total haemoglobin concentration in an area consistent with the contralateral motor and sensory cortex (fig 3). The amplitude of the measured increase was 25 mM—greater than the equivalent change observed using NIRS and optical topography.4,8 This is likely to reflect the improved spatial resolution and hence reduced partial volume effect of the three-dimensional imaging system.

{kind=link}
{kind=link}
{kind=link}
Sagittal slices across three-dimensional image of change in total haemoglobin concentration in an infant brain due to passive movement of the left arm, showing an increase near the estimated position of the right motor cortex (denoted by the cross). Reprinted from NeuroImage, 30, Gibson AP, Austin T, Everdell NL, et al. Three-dimensional whole-head optical tomography of passive motor evoked responses in the neonate, figure 4, p. 526, © 2006, with permission from Elsevier.
Current challenges with optical tomography
The biggest challenges in three-dimensional optical tomography are to improve quantitation and spatial resolution. Although the spatial resolution of optical tomography is not likely to match that of MRI, CT or ultrasound, it is probably comparable with positron emission tomography.
Improved resolution is possible by incorporating prior anatomical information from generic MRI scans of newborn infants and this approach is being actively pursued by our group at UCL. The current instrument is large and requires a team of physicists, engineers and computer scientists to operate and reconstruct the images. Work is underway at developing a smaller and faster instrument with data collection and reconstruction software that can be used by clinicians. Although difficult to predict the cost of a commercial instrument, it will probably be similar to that of other portable imaging tools, such as ultrasound.
FUTURE DEVELOPMENTS IN OPTICAL IMAGING
Over the past 25 years the clinical application of NIRS has been frustratingly slow.33 The challenge is to develop optical imaging systems into clinically useful cotside tools. Three-dimensional optical tomography represents a major advance in this field. Unlike functional MRI, optical images can be acquired in unsedated infants at the cotside; by measuring both oxyhaemoglobin and deoxyhaemoglobin independently it is possible to distinguish the increased oxygen extraction due to brain activation from changes in regional blood volume due to local vasodilatation. Measurements from deep inside the brain will allow cerebral maturation in the preterm brain to be investigated.
Optical imaging currently uses compounds that absorb natural light in the brain; however, it is equally sensitive to exogenous contrast agents.34 One can expect, with the development of new molecular optical imaging markers, optical tomography will be able to provide unique physiological images in vivo. This would represent a remarkable advance in the brain-oriented care of the newborn.
Acknowledgments
The author would like to thank the following members of the Biomedical Optics Research Laboratory and Institute for Women’s Health at UCL: Professor Jem Hebden, Dr Adam Gibson, Professor John Wyatt and Dr Judith Meek.
The work carried out at UCL was funded by grants from the Medical Research Council, Wellcome Trust and Engineering and Physics Research Council with support from University College London Hospitals NHS Foundation Trust.
Optical systems could be valuable tools for assessing cerebral function at the cotside
REFERENCES
Footnotes
-
Competing interests: None declared.