Article Text

Statistics from Altmetric.com
Neonatal airway management (NAM) and oxygenation are vital skills. Unrecognised oesophageal intubation is a common cause of endotracheal intubation (EI) failure and can result in mortality and significant morbidity. The Difficult Airway Society have algorithms for difficult airway management in adults and children1 ,2 including a ‘cannot intubate and cannot ventilate’ (CICV) algorithm.2 There are no nationally agreed guidelines or algorithms for NAM. The aim of this study is to determine NAM practises in UK level 3 neonatal intensive care units.
Between May and June 2013, a telephone survey of NAM, airway adjuncts and the possession of written NAM policies was undertaken in all UK level 3 neonatal units using a predetermined questionnaire.
All 59 units participated. All units used premedication for elective intubations. Suxamethonium was the most commonly used muscle relaxant along with an analgesic for sedation. Overall, 66% used colour-change capnography for endotracheal tube (ETT) placement confirmation. In all, 34% used them at every intubation. A total of 32% only used capnography if there was uncertainty about ETT position (low oxygen saturations and heart rate); 34% of units did not use capnography. In all, 53% limited the number of intubation attempts; two attempts was the most common limit set. Overall, 51% used oropharyngeal airways routinely; 68% had an emergency difficult airway kit, the contents of which varied (table 1). In all, 7% had a documented CICV policy.
Neonatal airway management and adjuncts used
This is the first review of UK NAM practices. The variation shown has potential for mismanagement of the neonatal airway. Capnography is standard adult practice and recommended by The Royal College of Anaesthetists and The Difficult Airway Society for every EI.3 Overall, performance of neonatal EI is poor with success rates being as low as 21%.4 ,5 Capnography for the confirmation of intubation success in neonates should be standard practice. During cardiac arrest, if exhaled CO2 is not detected, ETT position should be confirmed using direct laryngoscopy prior to commencing a new intubation attempt. Repeated laryngoscopies should be avoided as they can cause significant trauma to the airway.
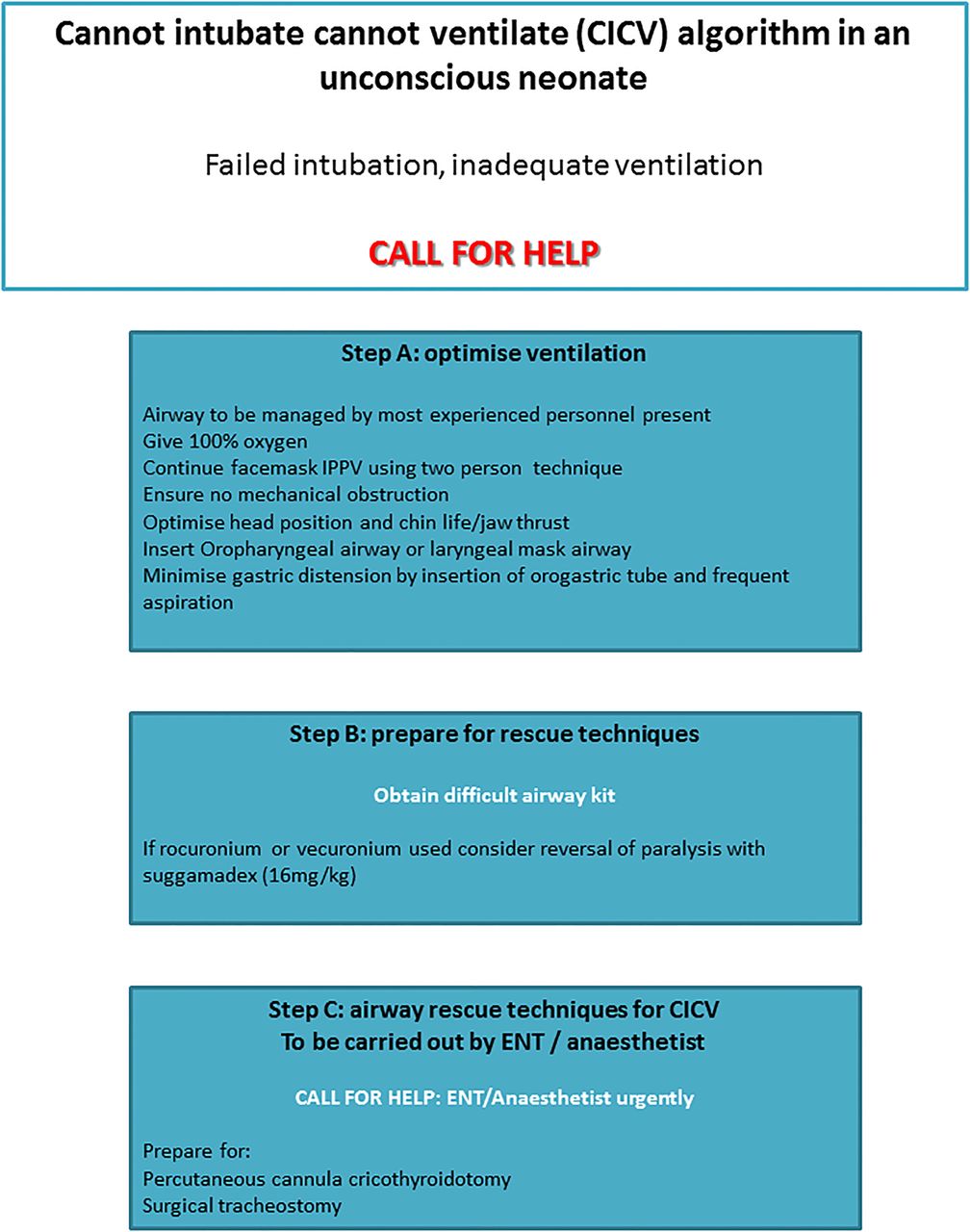
Human factors such as stress, poor communication, leadership, team working or inadequacy of equipment can all contribute to a poor outcome in a difficult airway situation. To prevent this, standardisation of practice with evidence based or consensus guidelines is warranted via documented airway management algorithms (suggested CICV algorithm: figure 1) and to avoid the inequality between neonatal and adult and paediatric airway management practices.
{kind=link}
Cannot intubate cannot ventilate algorithm in an unconscious neonate.
Acknowledgments
We would like to thank all those who participated in the survey.
Footnotes
-
Contributors FP and CD conceived the project. DJL and TW performed the data collection. FP performed data analysis. TW and FP wrote the draft manuscript. All authors reviewed and commented on the final draft of the paper. FP will act as the guarantor of the paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.