Article Text

Abstract
Objective The persistence of the patent ductus arteriosus (PDA) is frequently encountered in very preterm infants. Neither preventive nor curative treatments of PDA have been shown to improve the outcome of these infants. Since no consensus on optimal treatment of PDA is established, we evaluated the rate of spontaneous PDA closure in infants born before 28 weeks of gestation.
Patients and methods We studied a retrospective cohort of 103 infants (gestational age 24–27 weeks) admitted to our neonatal intensive care unit from 1 June 2008 to 31 July 2010. Maternal and neonatal characteristics were collected. The PDA was defined by the persistence of ductal patency after 72 h and was followed up by regular echocardiography.
Results Twelve infants died within the first 72 h and were excluded from the analysis. Among 91 infants analysed, 8 (9%) closed their ductus arteriosus before 72 h and the ductus could not be determined patent in 13. Of the 70 infants with a PDA still persistent, one underwent surgical ligation and echocardiography showed spontaneous closure in 51 (73%) of them. In the remaining 18 infants, the date of PDA closure could not be determined either because of their death (n=11) or due to discharge (n=7). Overall, a spontaneous closure of the ductus arteriosus was observed in 59 of the 91 infants.
Conclusions We have to question whether exposure to the risks of therapeutic interventions targeted for ductal closure is warranted since a PDA closes spontaneously in at least 73% of infants born before 28 weeks.
- Neonatology
- Intensive Care
- Therapeutics
Statistics from Altmetric.com
What is already known on this topic
-
Medical treatments by cyclooxygenase inhibitors for patent ductus arteriosus (PDA) closure are routinely employed in neonatal intensive care units.
-
Subsequent benefits of closing the PDA either medically or surgically in the preterm infant have not been demonstrated.
-
In the extremely preterm infant, the natural history of the PDA has not been studied because of the early administration of treatments targeting its closure.
What this study adds
-
Without any specific treatment aimed to close PDA, a spontaneous closure rate of 73% was observed in infants born before 28 weeks of gestation.
-
In the absence of evidence of improvements in outcome, exposure to the risks of therapeutic interventions targeted for ductal closure may not be warranted.
Introduction
The persistence of the patent ductus arteriosus (PDA) is frequent among preterm infants and its incidence is inversely proportionate to their gestational age at birth. Persistent PDA occurs in about two-thirds of extremely low-birth-weight infants,1 and 75% of those born before 28 weeks of gestation.2 Despite various randomised clinical trials conducted during the last three decades, there is no consensus on optimal treatment policy to achieve ductal closure in preterm infants. The efficiency of medical treatment by cyclooxygenase (COX) inhibitors (indomethacin, ibuprofen) on the closure of the PDA or on the resort to surgical ligation is well documented.3 Nevertheless, long-term benefits for the preterm infant other than those inherent to the treatment (ie, ductal closure or sparing surgical ductal ligation) remain uncertain and outcomes have not been shown to improve.4
Two meta-analyses confirm that prophylactic treatment by indomethacin or ibuprofen before 24 h of life has no impact either on the mortality, incidence of bronchopulmonary dysplasia (BPD) or adverse neurodevelopmental outcomes up to 36 months.5 ,6 However, indomethacin prophylaxis reduces the incidence of intraventricular haemorrhage (IVH) ≥grade 3 by 30%5 and early serious pulmonary haemorrhage by 35%.7 The decrease in the incidence of severe IVH has not been demonstrated with the use of ibuprofen prophylaxis for ductal closure.6 No reported clinical trials to date were designed to compare prophylactic treatment versus no treatment. Administration of either indomethacin or ibuprofen after 24 h achieves ductal closure in a lesser number of cases but is not associated with a reduction in mortality or in short-term outcomes such as BPD, severe IVH and necrotising enterocolitis (NEC) when compared with a placebo.8
In face of the risks associated with medical treatment and surgical ligation, some authors have questioned the benefits of treating the PDA either medically or surgically in the preterm infant.9 In clinical practice, treatment strategies vary from one neonatal intensive care unit (NICU) to another and several clinical teams have adopted a conservative or expectant treatment approach for the persistent patency of the ductus arteriosus.10 ,11 In the absence of clear benefits of either preventive or curative treatment demonstrated on mortality and morbidity, we evaluated the rate of spontaneous closure of the PDA without any specific treatment aimed at its closure in infants born before 28 weeks of gestation.
Patients and methods
All infants born between 240/7 and 276/7 weeks of gestational age and admitted to the NICU at Antoine-Béclère Hospital from 1 June 2008 to 31 July 2010, either inborn or outborn, were retrospectively included. During this period, our standard approach to treatment of PDA was conservative. We did not use any COX inhibitor for prophylactic or after 24 h treatment of PDA; mechanical ventilatory parameters were adjusted with a low inspiratory time (Ti: 0.30–0.35 s) and a high positive end expiratory pressure (PEEP=5 mbar); fluid intake was limited to less than 140 mL/kg/day beyond day 3 as much as possible.
Doppler echocardiography was performed with a GE Logiq 7 with a 10 MHz transducer (General Electric Healthcare, Vélizy-Villacoublay, France) before day 4 of life. The PDA was defined by the persistence of ductal patency after 72 h of life with a left-to-right shunt. PDA was considered to be haemodynamically significant (HSPDA) on the echocardiography carried out between 3 and 4 days of life when internal ductal diameter was above 1.5 mm and there was increased pulmonary output documented by an end-diastolic flow velocity in the left pulmonary artery (LPA) measured by pulsed Doppler above 0.2 m/s or a left-atrium-to-aortic-root (LA/Ao) ratio above 1.5.12 All PDAs were followed up by regular echocardiography (once or twice a week), and when it showed the ductus to be closed, the date of the echocardiography was considered as the ductal closure date. The absence of spontaneous closure in a large-sized PDA with increased pulmonary output (LA/Ao ratio above 1.8 and an end-diastolic LPA velocity above 0.2 m/s) in the context of severe respiratory failure was treated by a surgical ligation of the PDA.
For all infants included, we collected the following data:
-
Maternal and perinatal characteristics including antenatal corticosteroid therapy, mode of delivery and the cause of preterm delivery (preeclampsia, chorioamnionitis, isolated premature rupture of membranes and isolated preterm labour).
-
Neonatal characteristics: sex, birth weight and being small for gestational age defined by a birth weight below the 10th centile of the French standards (AUDIPOG).13
-
Respiratory outcomes: number of exogenous surfactant doses administered, pulmonary haemorrhage, mechanical ventilation (through an endotracheal tube) and nasal intermittent positive pressure ventilation (IPPV) or continuous positive airway pressure (CPAP) duration before discharge. At 36 weeks postmenstrual age (PMA), the result of the Walsh test was used to define BPD.14
-
Neurological outcome: the most severe grading of the IVH picked up by a cranial ultrasound scan (CUS) carried out in the first 15 days of life was recorded. We have used the classification of IVH as described by Volpe.15
-
NEC and spontaneous intestinal perforation.
-
Duration of hospitalisation on NICU in days.
In case of death, its cause was recorded.
Data handling and statistical analysis were performed using the software ‘Biostatgv’ (Université Pierre-et-Marie-Curie, Paris, and Université Paul Sabatier, Toulouse, INSERM http://www.u707.jussieu.fr/biostatgv/). The comparative statistical analysis between groups was carried out by a non-parametric Fisher's test with a significant threshold of <0.05 for the p value.
Results
We identified 103 infants born between 240/7 and 276/7 weeks of gestational age, admitted to the NICU from 1 June 2008 to 31 June 2010. Twelve infants died in the first 72 h and were thus excluded. Three of them were born at 24 weeks, 6 at 25 weeks, 2 at 26 weeks and 1 at 27 weeks of gestation. The causes of death were four early-onset neonatal infections, two hypoxic respiratory failures non-responsive to inhaled nitric oxide, three pulmonary haemorrhages (two on day 1 and one on day 2 of life), one bilateral periventricular haemorrhagic infarction (PVH) in the first 24 h, one lung hypoplasia and one multiple congenital abnormalities.
Ninety-one preterm infants were analysed; their characteristics are listed in table 1. The average maternal age was 30.6±5.4 years, and the pregnancy was multiple in 21% of cases. A complete course of antenatal corticosteroid therapy was administered in two-thirds of cases. A single dose of betamethasone was received by 25% of women and in 10% of them there was no antenatal corticosteroid therapy. The prematurity was secondary to chorioamnionitis in 47% and to preeclampsia in 18% of cases, followed by isolated preterm labour in 24% and was related to isolated premature rupture of membranes in 9% of cases.
Perinatal and neonatal characteristics
Exogenous surfactant was administered once to 55 infants (60%), twice in 29 infants (32%) and a third dose was given to 6 of them. Pulmonary haemorrhage was observed in 25% (23/91) of infants. The average length of mechanical ventilation and non-invasive respiratory support (nasal IPPV or CPAP) were of 26±19 days (from 2 to 87 days) and 36±21 days (from 3 to 168 days), respectively. At 36 weeks PMA, the rate of BPD was of 35%. A CUS performed in the first two weeks of life found an IVH grade ≥3 in 19 infants (21%). No retinopathy of prematurity (ROP) was found before discharge.
The average admission days on the NICU were 73±34 days (from 23 to 204 days). Fifteen infants died after 72 h of life. Five of them were born at 24 weeks, 4 at 25 weeks, 4 at 26 weeks and 2 at 27 weeks of gestation. The causes of death were one pulmonary haemorrhage, two hypoxic respiratory failures, one lung hypoplasia, two pneumothoraxes one of which was secondary to lung hypoplasia related to prolonged anamnios, one septic shock following nosocomial infection, three grade 3 IVHs with associated PVHs, two NECs, two multisystem failures and one oesophageal atresia. An ethical discussion among the medical staff and with the parents resulted in decisions of treatment withdrawal taken for four of these deaths (the three severe IVHs and the oesophageal atresia).
Of the 91 infants included, 8 (9%) closed their ductus arteriosus spontaneously before 72 h of life and in 70 of them the PDA persisted beyond 72 h (figure 1). The infants in whom the ductal closure occurred before 72 h were born at an average gestational age of 270/7 weeks±5 days, whereas those with a persistent PDA were born at an average gestational age of 262/7 weeks±7 days. In 13 infants, the persistence of the PDA was not assessed by echocardiography after the first week of life. Three of them died at day 4, day 11 and day 12 of life, respectively. The remaining 10 infants were free of respiratory support at an average age of 7±6 days (from 2 to 20 days), and none of them had a positive Walsh test at 36 weeks PMA.

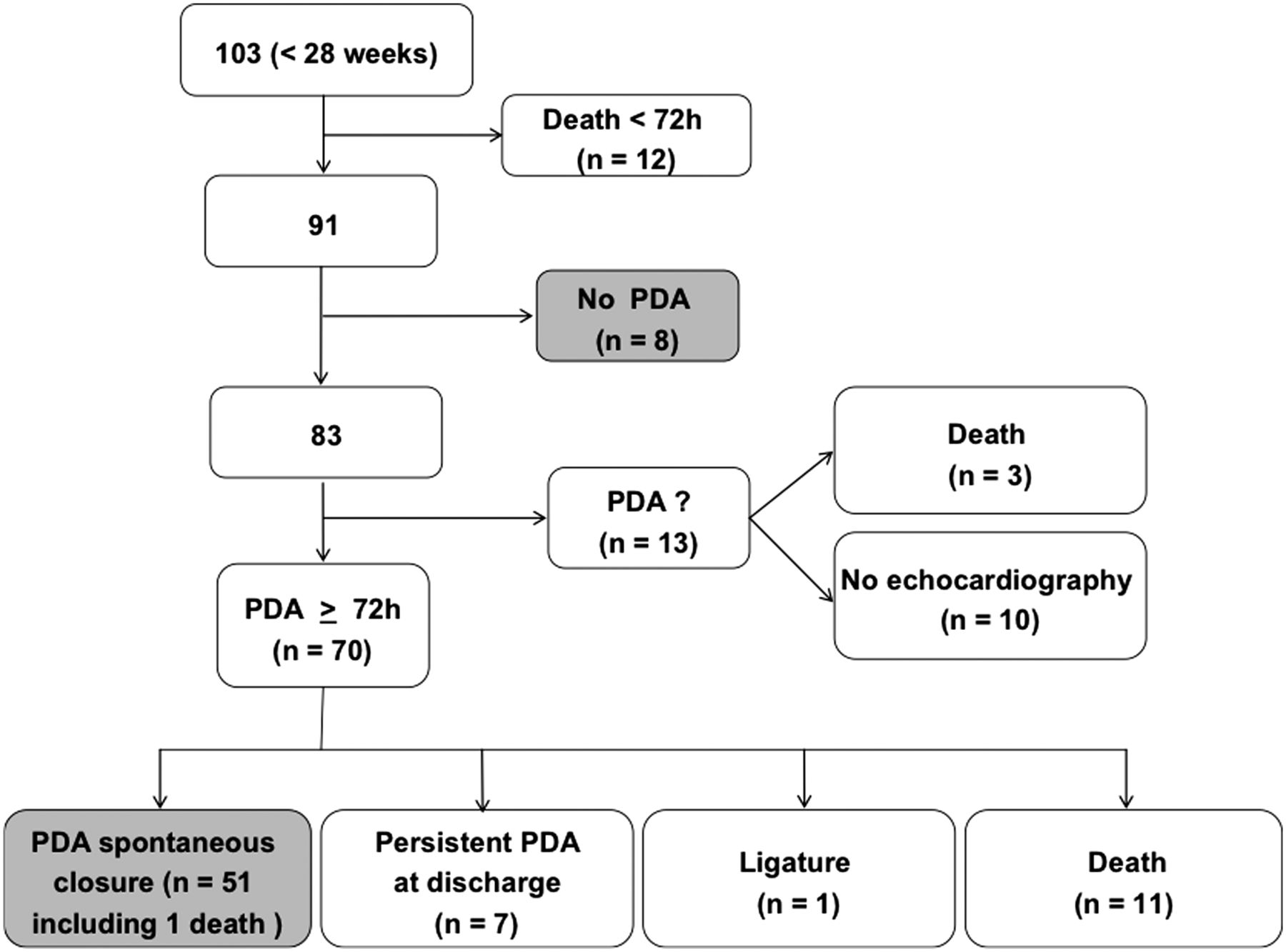{kind=link}
Natural evolution of patent ductus arteriosus in a population of infants born before 28 weeks of gestation.
Of the 70 infants with a PDA, echocardiography showed spontaneous closure in 51 infants (73%) at an average age of 61±37 days (from 4 to 165 days). Only one infant underwent surgical ligation of the PDA. In the remaining 18 infants, the date of PDA closure could not be determined either because of their death (n=11) or because the echocardiography before discharge showed the PDA to be still persistent (n=7). Three of them were later seen in follow–up, and the reviewing paediatrician found no heart murmur. The other four were transferred to another neonatal service before being discharged home. Overall, a spontaneous closure of the ductus arteriosus was confirmed by echocardiography in 59 of the 91 infants (65%) and in 58 of the 76 (76%) surviving infants.
Of the 28 infants born at 24–25 weeks, 25 (89%) were found to have a PDA compared with 45 of 63 (71%) infants born at 26–27 weeks. The observed spontaneous PDA closure rate was 60% (15 of 25) in infants born at 24–25 weeks compared with 80% (36 of 45) in those born at 26–27 weeks. The rates of PDA occurrence or its spontaneous closure for infants born at 24–25 vs 26–27 weeks were not significantly different.
The evolution of a PDA towards spontaneous closure with regards to its haemodynamic significance as established by Doppler echocardiography is represented in table 2. In 17 cases, the documented data did not allow us to determine the haemodynamic status of the PDA. The spontaneous closure rate was observed in 78% (18 of 23) of the infants with an HSPDA and in 73% (22 of 30) of those with a haemodynamically non-significant one. This difference was not statistically significant.
Evolution of persistent patent ductus arteriosus (n=70) according to their haemodynamic characteristics at 3–4 days of life
Discussion
In the extremely preterm infant, the natural history of the PDA has not been studied because of the early administration of treatments targeting its closure. Among preterm infants, 70% of those born before 28 weeks of gestation receive either medical or surgical therapy for PDA closure.16 To justify the early use of these treatments on preterm infants in whom the PDA would possibly close spontaneously, the following two conditions seem necessary to us. First, it must be effective and its efficiency must be demonstrated not only on the closure of the PDA but also on mortality and long-term outcomes. Second, the clinical consequences of a persistent PDA must be more important than the risks undertaken by its treatment. The efficiency of medical treatment by COX inhibitors for PDA closure has been proved by numerous studies, but its efficacy depends on the age of the infant at the time of its administration.3 ,17 A prophylactic medical treatment in the first 24 h of life gives better results on ductal closure compared with a later treatment. In 257 infants born between 24 and 27 weeks, PDA closure was observed in 97% of infants treated before 15 h of life and in 51% of infants treated for an HSPDA at day 3 of life.2 In case of failure of medical treatment, a surgical intervention may be proposed. However, the surgical ligation has been described to possibly increase the risk of poor long-term outcomes in these extremely preterm infants.18 A recent study examined the effects of a ‘conservative’ approach towards a PDA persistent after one or two courses of indomethacin. In the group having systematically a surgical ligature of their PDA, the rate of NEC was higher than in the group operated on only in case of an HSPDA.19 For these different reasons, we have chosen a conservative attitude towards the PDA in treating it only if it has immediate deleterious clinical consequences.
In our study, we observed a spontaneous closure of the PDA in 73% of infants born before 28 weeks and a 9% early spontaneous closure rate defined as closure of ductus arteriosus before 72 h of life. Narayanan et al2 found a spontaneous ductal closure rate of 27% at day 4 in 143 infants born between 24 and 27 weeks. This last study described also a variable rate of spontaneous ductus closure according to the gestational age at birth with a rate of 31% among the infants born between 26 and 27 weeks and of 21% among those born between 24 and 25 weeks. Without limiting ourselves to the ductal closure during the first few days of life, our study did not show any significant difference in the spontaneous PDA closure rate between the infants born at 24–25 weeks and 26–27 weeks (60% vs 80%). Finally, we did not observe the spontaneous PDA closure to be more frequent in infants with regards to the haemodynamic significance of the PDA (78% vs 73%).
In case of persistence of the PDA beyond the first few days of life, a later closure may occur. Herrman et al20 showed that 86% of very low-birth-weight infants with a PDA persistent at discharge spontaneously closed their PDAs at an average of 51 days of life. In our population of extremely preterm infants, we observed PDA closure at an average of 61 days of life with a large variation.
We cannot exclude that our conservative management of PDA may have resulted in an increased mortality. Four of the 12 deaths that occurred before the first 72 h were due to three severe pulmonary haemorrhages and one IVH-PVH, which could not have been prevented even with a prophylactic treatment of PDA. However, among the 15 deaths that occurred after 72 h, one severe pulmonary haemorrhage and three severe IVH-PVHs could be related to the absence of very early treatment to close the PDA. The 17% rate of mortality observed in our population was higher than the 12% reported by Jhaveri et al19 in infants born before 28 weeks and treated by prophylactic indomethacin for ductal closure. For comparison with this last population, we have observed a higher rate of IVH grade ≥3 (21% vs 9%), a similar rate of BPD at 36 weeks PMA (35% vs 32%), and a lower rate of NEC (3% vs 16%) and ROP ≥ 2 (0% vs 14%).
Conclusion
Many therapeutic trials concerning the use of COX inhibitors used as either preventive or curative treatment of the PDA have been published in the last 30 years without any conclusion on either their short-term or long-term benefits.21 ,22 Currently, in the absence of tangible evidence regarding the efficiency of these treatments targeted for ductal closure on the mortality or short-term and long-term outcomes, we have to question these practices all the more so as a PDA closes spontaneously in at least 73% of infants born before 28 weeks of gestation.
References
Footnotes
-
Contributors Conception and design of the work: VZ-S and PB. Acquisition of data, analysis and interpretation of data: AR, SS-A, DD, VZ-S and PB. Drafting the article or revising it critically for important intellectual content: AR, SS-A, DD, VZ-S and PB. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: AR, SS-A, DD, VZ-S and PB.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms